




by the World Mercury Project
Related Epidemics? Teen Mental Health Crisis & Neurodevelopmental Disorders.
It has never been easy to be an adolescent, but by the look of things, twenty-first century teenagers may be having a harder time than ever.
One contributing factor—the one that public health agencies and the media seem most willing to discuss—is a ballooning epidemic of mental health problems in teens.
Meanwhile, an equally grim developmental disability crisis has been unfolding for years, affecting at least one in six American children and teens but receiving little attention.
Officialdom’s subtle sidelining of developmental disorders in favor of a focus on mental health is somewhat baffling, given that researchers frequently use the terms “neuropsychiatric” and “neurodevelopmental” interchangeably.
This is particularly the case when they refer to diagnoses such as attention-deficit/hyperactivity disorder (ADHD) and other behavioral disorders.
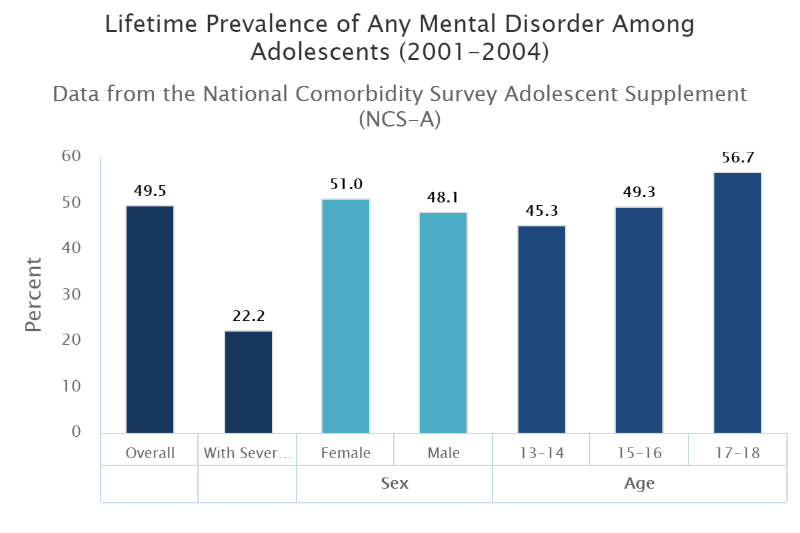
In fact, one of the most credible national surveys cited as evidence of the teenage mental health crisis (called the NCS-A and published in the Journal of the American Academy of Child & Adolescent Psychiatry in 2010) defines three behavior disorders (ADHD, conduct disorders and oppositional defiant disorders) as “mental disorders.”
…half (49.5%) of U.S. teens ages 13-18 suffered from at least one mental disorder…
The NCS-A was conducted with over 10,000 teens from 2001-2004. The survey found that half (49.5%) of U.S. teens ages 13-18 suffered from at least one mental disorder (see chart), including one in five with behavior disorders and three in ten with anxiety disorders.
The age of onset for the disorders often preceded adolescence by many years (for example, half of affected adolescents developed their anxiety disorders at age 6).
Additionally, the impairments were often severe, ranging from 22.2% to 27.6% of teens, which is striking given that the survey measured “higher thresholds of impairment that required endorsement of ‘a lot’ or ‘extreme’ impairment in daily activities, or ‘severe or very severe’ distress.”
Acknowledging that its own mental health surveillance data have significant limitations, the Centers for Disease Control and Prevention (CDC) praised the NCS-A because of its unique focus on childhood mental disorders and its inclusion of disorders not measured in other studies.
What are the likely culprits?
Regardless of specific terminology, one burning question arises: why do children and teens currently have such high levels of mental and neurologic dysfunction?
Although the pro-Pharma health care system in the U.S. makes it socially taboo to say so, vaccines and other pharmaceutical products are some of the most likely culprits.
As has been discussed in other World Mercury Project articles about children’s health, this supposition is backed by sound science.
For example, two epidemiological studies from 2017 are suggestive of temporal associations between vaccines and subsequent pediatric disorders:
- Researchers from the Yale Child Study Center published a retrospective case-control study in Frontiers in Psychiatry that considered whether prior vaccination in a national sample of privately insured children and adolescents (ages 6-15) was associated with increased incidence of seven neuropsychiatric disorders. For the time period from January 2002 through December 2007, the Yale researchers found that children with four diagnosed disorders—anorexia nervosa (AN), anxiety disorder, tic disorder and obsessive-compulsive disorder (OCD)—were more likely than matched controls to have received a flu shot in the preceding 12 months. There were also associations between prior receipt of several other vaccines (hepatitis A, meningococcal and Td) and some of the neuropsychiatric diagnoses.
- A prospective case-control study published in Brain Injury used the Vaccine Safety Datalink database to zero in on the relationship between thimerosal-containing vaccines given in the first six months of life (for children born between 1991 and 2000) and the long-term risk of diagnosis with “disturbance of emotions specific to childhood and adolescence,” a diagnostic category abbreviated as ED. The results showed a significant relationship between vaccine-related mercury exposure and the subsequent risk of an ED diagnosis, with a notable dose-response effect. As a side comment, the authors note that occupational health specialists have recognized depression and other psychological disturbances as symptoms of mercury poisoning for decades.
Other recent research observes that exposure to neurotoxic and excitotoxic vaccine ingredients (such as thimerosal, aluminum adjuvants and monosodium glutamate) can lead to changes in the brain, adversely affecting the long-range connectivity that makes it possible to pay attention and engage in big-picture thinking.
This abnormal connectivity is a key feature not only of ADHD but of leading neurodevelopmental conditions such as autism spectrum disorder (ASD) and tic disorders.
The pharmaceutical connection
A TIME article on the “startling” rise in teen depression laments the fact that there has not been “a corresponding increase in mental health treatment for adolescents and young adults.”
This prospect of a vast untapped market for greater pharmaceutical sales may offer one clue as to why many powerful organizations are focusing on the mental health aspects of teenagers’ wider health crisis.
However, other evidence indicates that some pharmaceutical products (in addition to vaccines) may be contributing to mental health problems. A Psychology Today report notes that,
“aggressive marketing by drug companies…has transformed mild depression and even sadness into a disease of ‘serotonin deficiency.’”
At the same time, there has been growing awareness of,
“the potential for certain prescription medications to increase the risk of psychiatric symptoms and suicidality.”
Classes of medications that come with black box warnings mandated by the U.S. Food and Drug Administration (FDA) include some of the very drugs used to address both psychiatric and neurological conditions, such as antidepressants and antiepileptics.
In 2009, the FDA added warnings for the class of drugs known as leukotriene inhibitors (LTIs), which clinicians recommend for the control of allergies and asthma.
Although sales of LTIs abruptly dropped as soon as the warnings appeared, the cautions did not manage to save an 18-year-old asthmatic who recently committed suicide after taking an LTI.
The CDC tells us that,
“mental disorders among children are an important public health issue because of their prevalence, early onset, and impact on the child, family, and community.”
When an adolescent is too incapacitated by a mental or neurological disorder to pursue his or her education or a career, the whole country loses. Young people’s brains and emotions get plenty of a workout just by engaging in the process of growing up.
Piling on more brain-scrambling pharmaceutical products to treat conditions that are often iatrogenic to begin with is probably not what most teenagers need.
Related Teen Epidemics? Looking for Answers in All the Wrong Places
As discussed in Part One (above), American teenagers are drowning in a rising tide of disorders: behavioral issues, sensory problems, depression, self-harm and more.
The medical-pharmaceutical industry has rushed to brand all of these problems as mental health conditions treatable with profit-generating drugs. Few are talking about the broader neurodevelopmental crisis—triggered in part by environmental toxins such as the mercury and aluminum in vaccines—that is sabotaging children’s neurodevelopment and sapping adolescent resilience.
Age of Autism’s media editor Anne Dachel deconstructs this disproportionate focus on mental health, suggesting that the underlying aim of proclaiming half of American children mentally subpar may be to mask the real and serious neurological issues affecting children. As Dachel explains,
“If every other child is ‘mentally ill,’ the ones with autism…and a host of developmental problems won’t matter.”
In short, mental illness will become “a normal and acceptable part of childhood,” conveniently letting the manufacturers and purveyors of environmental toxins off the hook.
Blame the parents—for everything
Dachel astutely observes that some of the trendiest explanations for teen distress are inherently victim-blaming—or, more precisely, parent-blaming.
Chief among these is the suddenly ubiquitous notion that teens’ problems are all due to “adverse child experiences” (ACEs), a vaguely conceptualized term comprising early-life trauma or abuse and household dysfunction.
The sweeping line of reasoning underlying ACE research is that experiences such as “trauma exposure, parent mental health problems and family dysfunction put children at risk for disrupted brain development and increased risk for later health problems and mortality.”
In response, researchers are calling for a more “trauma-informed and trauma-focused” approach to psychiatric diagnosis and treatment. Investigators also have begun holding ACEs responsible for a wide range of health behaviors and outcomes, including “depressive symptoms, ADHD symptoms, cigarette use, alcohol use, marijuana use, and BMI, in addition to lower levels of fruit and vegetable intake, and sleep.”
Without discounting the potential mental and physical health impacts of trauma and abuse, there are two problems with using ACEs as a catch-all explanation for young people’s mental and neurodevelopmental woes.
First, a large body of scientific evidence clearly indicates that the neurodevelopmental disorders disabling today’s youth are multifactorial in origin.
ACEs are only one component of a much longer list of likely environmental factors—including chemical pollutants and drugs—that can “interfere with typical brain developmental trajectories, eventually increasing the risk of either subclinical neuropsychological alterations or…clinical conditions such as learning disabilities, autism spectrum disorder (ASD) and attention deficit/hyperactivity disorder (ADHD).”
Second, it is hard to explain why ACEs suddenly should result in sky-high rates of intellectual disabilities and developmental delays (including autism) when, historically, even the most extreme forms of adversity have not been predictive of neurodevelopmental disorders. As Dachel observes,
“Adversities and stress are nothing new. Somehow, everyone’s buying into the idea that kids today are falling apart because of the stress of modern life.”
Dachel describes her grandfather’s family, which left Northern Ireland after going through a lot in the struggle for independence. She observes,
“He and his siblings were working at a very young age when they got to North America. Although no one went beyond the fourth grade and they were as poor as one can imagine, all these kids were normal, intelligent and functional. They had to function in the adult world, and they did it.”
As with refugees from the Northern Irish “troubles,” there is no evidence that Holocaust survivors had (or have, for those still alive today) higher rates of ADHD, Asperger’s, autism, learning disabilities, sensory processing disorders or dyslexia, despite undergoing extreme trauma.
Violinist Alison Fujito notes that Holocaust survivors
“were tortured and suffered emotional and physical agony, and most had severe nutritional deficiencies. Post-traumatic stress disorder (PTSD) is the norm for a Holocaust survivor, not the exception.”
Yet after Fujito’s father escaped Nazi-occupied Austria, leaving
“his home and his entire family at age 14, not knowing if he’d ever see his parents, aunts, uncles or cousins again—talk about stress!—he hardly ever got sick, and it certainly didn’t affect him neurologically. He earned top honors in an English-language school though his first language was German and went on to not one but two successful careers. And he was always happy and cheerful—this was not an act, he was just a positive force.”
Fujito noted that Holocaust survivors also
“didn’t have fidget toys.”
If it’s not the parents, it’s the smartphones
Dachel’s commentaries note that, in addition to ACEs, a growing number of celebrities and academics are blaming smartphones and social media for adolescents’ plummeting mental health.
Again, without discounting this still-emerging body of research, the chronological sequence of events suggests that this can only be a partial answer at best. The first mass-market-oriented smartphone did not appear on the scene until 2007, and widespread smartphone ownership did not take off until some years later.
However, rates of neurodevelopmental disorders started climbing in the 1990s, and the widely cited national survey that first highlighted the astoundingly high prevalence of teenage mental health disorders was conducted in 2001-2004.
Unhelpful victim-blaming explanations serve corporate interests, allowing powerful medical and pharmaceutical entities to shirk their ethical responsibilities.
Instead of telling parents they are doing everything wrong, we should immediately be looking to reduce children’s and teens’ exposure to neurotoxins and other damaging chemical concoctions.
Otherwise, families, schools and communities increasingly will find themselves hard-pressed to fulfill their task of safely guiding adolescents into a healthy and happy adulthood.
Read all of part 1 here, and part 2 here, at WorldMercuryProject.org.

Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?

One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.

Leave a Reply