




The live oral polio vaccine is so easy to administer, it is often given to children right on the streets in poor countries, without even checking whether or not they have already received it. Photo by UNICEF.
by Christina England
Health Impact News
Vaccine Derived Polio Victim Excretes Polio Virus for 28 Years
Scientists state that there have been no cases of wild polio reported in four out of the six regions being targeted in the vaccine-program since the 1990s, and the only cases of polio that are being reported are those of VDPV caused by the OPV vaccination.
Many people are unaware that polio infections do not always lead to paralysis. In fact, according to the renowned board certified pediatrician, Dr. Lawrence B. Palevsky, temporary or full paralysis is rare and is only seen in two percent of cases because the majority of polio infections cause little more than a simple case of gastroenteritis.
In response to an article published in The Telegraph India, Dr. Palevsky wrote:
The oral polio vaccine was banned from use in the United States in 2000. The reason for this ban was because too many children were developing vaccine associated paralytic polio (VAPP) as a serious side effect of the oral vaccine. In other words, they were developing paralytic symptoms that the vaccine was supposed to prevent them from developing, should they have gotten a natural polio infection and developed temporary or permanent paralysis, which are rare side effects of the polio illness anyway.
He stated:
When you hear about ‘outbreaks’ of polio in foreign countries, the first question you should ask is, ‘Are they using the oral polio vaccine?’ and the answer is usually, ‘yes.’ If children in the US were getting VAPP as a significant side effect of the oral vaccine, why wouldn’t this occur in other countries where children are receiving the oral polio vaccine, and health conditions may actually be worse for them there, than they are in the US? (own emphasis)
Unsurprisingly, the World Health Organization (WHO) has known about this for years, therefore you would think that they would have banned this dangerous vaccine. However, instead of banning this vaccine as one would expect, they have vowed to keep using the vaccine until wild polio virus has been eradicated. They stated:
Despite its many advantages, OPV carries the risk of vaccine-associated paralytic poliomyelitis (VAPP) particularly among infants who receive the vaccine for the first time and their contacts. In addition, when polio vaccine coverage is low in the population, this live attenuated vaccine may revert its virulence and transmissibility and pose additional risk for emergence of vaccine-derived polioviruses (VDPVs), which have been associated with outbreaks. Because of these risks, OPV use will be discontinued worldwide once the goal of eradicating all wild poliovirus (WPV transmission) is achieved.
Sadly, the result of their decisions has been catastrophic.
One Individual with VDPV Sheds Polio Virus for 28 Years
Polio is spread from person to person by coming into contact with infected feces. It is a known fact that in many parts of the developing world, sanitation is poor and water supplies are often contaminated with bacteria and raw sewerage, therefore, the spread of the disease is inevitable.
In August 2015, a team of scientists from the UK, led by Dr. Glynis Dunn, published a paper titled Twenty-Eight Years of Poliovirus Replication in an Immunodeficient Individual: Impact on the Global Polio Eradication Initiative. Their paper exposed the devastating effect that the WHO’s decision is having on the developing world.
They opened their paper by stating that:
Poliovirus strains in the oral vaccine are known to quickly revert to neurovirulent phenotype following replication in humans after immunisation. These strains can transmit from person to person leading to poliomyelitis outbreaks and can replicate for long periods of time in immunodeficient individuals leading to paralysis or chronic infection, with currently no effective treatment to stop excretion from these patients.
Dunn and her team continued by describing the case of one individual who has been excreting the poliomyelitis virus ever since receiving the OPV vaccine in 1986, a total of twenty-eight years.
No Wild Polio Cases Reported in Four Out of Six Regions

The scientists stated that there have been no cases of wild polio reported in four out of the six regions being targeted in the vaccine-program since the 1990s, and the only cases of polio that are being reported are those of VDPV caused by the OPV vaccination:
Four of the six WHO regions have been certified polio-free and a country such as India, where massive poliomyelitis outbreaks were very common, interrupted circulation of endemic wild poliovirus in 2010. There has been no case of poliomyelitis caused by circulating wild type 2 poliovirus since 1999, no case of type 3 since November 2012 and the last case of type 1 in Africa was in August 2014, leaving some areas of Pakistan and Afghanistan as the main remaining reservoirs. All type 2 poliomyelitis cases since 1999, except an isolated incident of 10 cases linked to a wild laboratory reference strain in India, are due to vaccine-related poliovirus strains in either recipients, their immediate contacts or after the vaccine virus has regained the ability to transmit and circulate freely.
The team believed that the continuing cases of polio that are being spread from VDPVs could be eradicated if the WHO was using the inactivated polio vaccines as opposed to live polio vaccines.
(Inactivated vaccines are those vaccines containing viruses that have been killed during the manufacturing process. See Inactivated whole-cell (killed antigen) vaccines.)
They concluded that:
Of the total of 73 iVDPV (immunodeficiency-related vaccine-derived poliovirus) cases that have been described between 1962 and 2014, only seven of them involved infections lasting more than five years. The case described here represents the only individual of those seven known to be excreting at present. However, several highly drifted VDPV strains have recently been isolated from sewage samples in Slovakia, Finland, Estonia and Israel. They included examples of all three poliovirus serotypes, although type2 VDPVs were the most prevalent among them. These VDPV isolates showed molecular properties typical of iVDPVs described above indicating that an unknown number of these chronic excreters exist elsewhere.
Their paper is extremely worrying and raises the question as to whether or not the continuing polio outbreaks being described in mainstream media are caused not by the polio virus but by contaminated feces.
Science Dictates that the Polio Virus Can Never be Eradicated
In 2012, Neetu Vashisht, and Jacob Puliye published a paper in the Indian Journal of Medical Ethics titled Polio programme: let us declare victory and move on. Throughout their paper they make it abundantly clear that polio is here to stay and that cases of vaccine induced polio are reaching an all time high. They wrote:
It was hoped that following polio eradication, immunisation could be stopped. However the synthesis of polio virus in 2002, made eradication impossible. It is argued that getting poor countries to expend their scarce resources on an impossible dream over the last 10 years was unethical.
Furthermore, while India has been polio-free for a year, there has been a huge increase in non-polio acute flaccid paralysis (NPAFP). In 2011, there were an extra 47,500 new cases of NPAFP. Clinically indistinguishable from polio paralysis but twice as deadly, the incidence of NPAFP was directly proportional to doses of oral polio received. Though this data was collected within the polio surveillance system, it was not investigated. The principle of primum-non-nocere was violated.
In other words, the oral polio vaccine is believed to be directly responsible for NPAFPs. Furthermore, according to their paper, the eradication of polio is impossible for the following reasons:
The charade about polio eradication and the great savings it will bring has persisted to date. It is a paradox, that while the director general of WHO, Margret Chan, and Bill Gates are trying to muster support for polio eradication, it has been known to the scientific community, for over 10 years, that eradication of polio is impossible. This is because in 2002 scientists had synthesised a chemical called poliovirus in a test-tube with the empirical formula C332, 652H492, 388N98, 245O131, 196P7, 501S2, 340. It has been demonstrated that by positioning the atoms in sequence, a particle can emerge with all the properties required for its proliferation and survival in nature. Wimmer writes that the test-tube synthesis of poliovirus has wiped out any possibility of eradicating poliovirus in the future. Poliovirus cannot be declared extinct because the sequence of its genome is known and modern biotechnology allows it to be resurrected at any time in vitro. Man can thus never let down his guard against poliovirus. Indeed the 18-year-old global eradication campaign for polioviruses will have to be continued in some format forever. The long promised “infinite” monetary benefits from ceasing to vaccinate against poliovirus will never be achieved. The attraction that ‘eradication’ has for policy makers will vanish once this truth is widely known.
The fact that we are being lied to is even more disturbing when you consider their data identifies that the children who contract NPAFP are twice as likely to die of their debilitating illness as from the wild polio virus.
Neetu Vashisht and Jacob Puliye wrote:
Sathyamala examined data from the following year and showed that children who were identified with non-polio AFP were at more than twice the risk of dying than those with wild polio infection.
They concluded that:
… Though all the data was collected within an excellent surveillance system, the increase was not investigated openly. Another question ethicists will ask, is why champions of the programme continued to exhort poor countries to spend scarce resources on a programme they should have known, in 2002, was never going to succeed.
Give Polio a New Name and Announce Eradication
Many professionals believe that Neetu Vashisht and Jacob Puliye are correct and blame the oral polio vaccine for cases of NPAFP. Other professionals, however, believe that polio has simply been renamed acute flaccid paralysis (AFP) to give the illusion that the disease has been eradicated.
While AFP is symptomatic of polio, it can be caused by other diseases such as Guillain-Barre syndrome and nerve lesions. (See India to get polio-free status amid rise in acute flaccid paralysis cases.)
Mr. Ron Law, a risk and policy adviser, believes that since India’s last official case of polio, there have been over 170,000 cases of AFP, which he says, prior to the vaccination campaign, were included in the polio diagnosis.
Explaining his views further, in a response to professor David Colquhoun’s paper published in the British Medical Journal, he wrote:
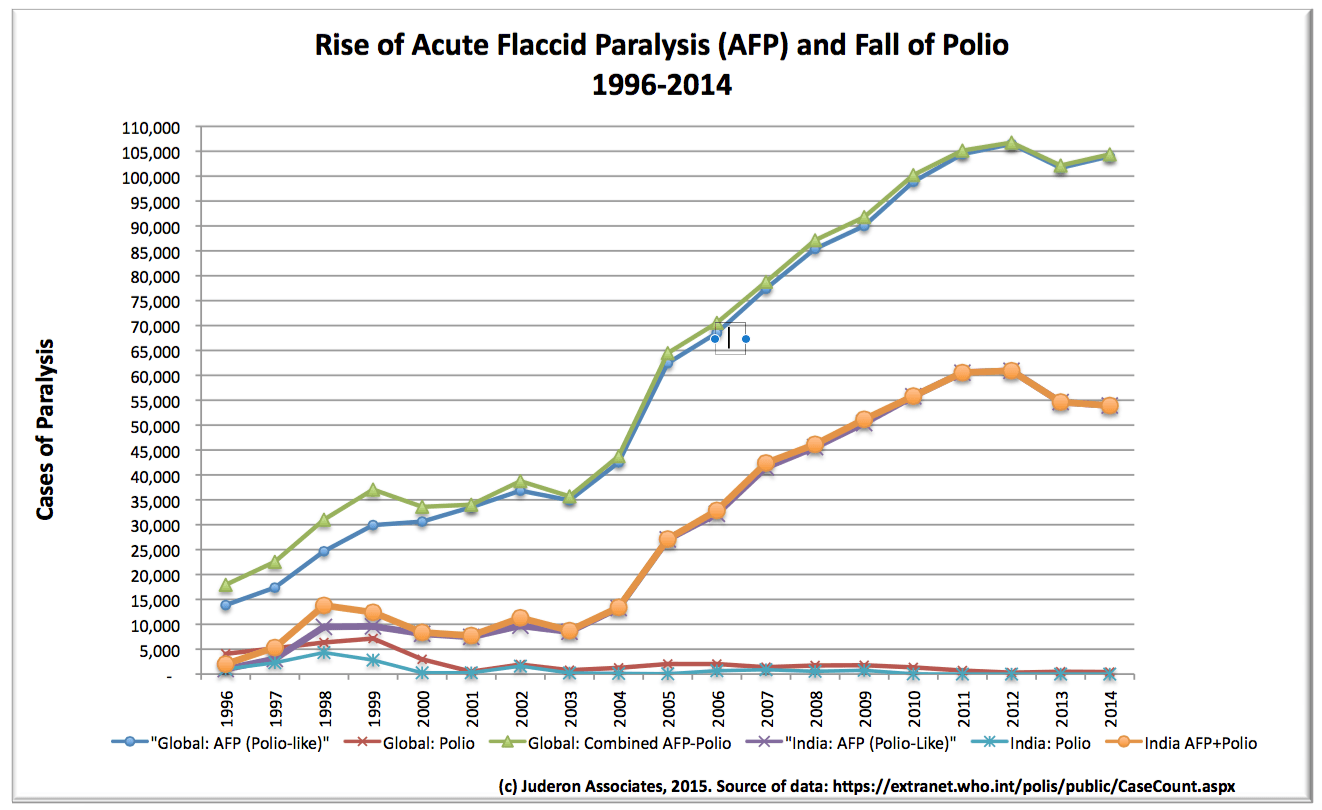
In 1995 India was claimed to have 30,000 cases of paralytic polio in children every year. A polio eradication programme was instigated with previous cases diagnosed as polio renamed Acute Flaccid Paralysis, or polio-like paralysis, with cases being screened for polio infection and only polio positive cases being called polio… the other clinically identical paralysis cases were classified as AFP.
The good professor implies that polio is no longer rampant.
Mr. Law stated:
Given that the WHO has recently announced to all and sundry that India is now officially polio free, let’s look at the WHO’s own data, from their website.
Despite claims that there were 30,000+ cases of polio in 1995, only 1,005 cases of AFP were notified in 1996, all of them being diagnosed as polio. In 2011, there were 60,849 cases of clinically diagnosed polio-like paralysis, one of which was confirmed as polio…
No doubt Professor Colquhoun is celebrating the wonderful success of the polio vaccination programme in India where children still got polio until recently even after having 30 plus polio vaccinations.
I wonder if redefining what was called polio before the vaccination eradication programme to AFP, or polio-like paralysis is what the good professor would call a medical success?
I suspect the parents of the 60,848 mostly vaccinated children (up to 30+ polio vaccine doses) paralysed by a polio-like illness will be rejoicing that polio is no longer rampant… that’s 252,000 children diagnosed with polio-like paralysis in the past five years.
He concluded:
And the good professor rests his case that polio is no longer rampant while reclassified polio-like paralysis continues unabated.
Perhaps the good professor could explain how reclassifying a disease and then claiming eradication of the disease is a medical success? Is that what he means when he said that medicine has moved on?
Mr. Law’s graph at the end of his response certainly added weight to his theory.
To update Health Impact News further, Mr. Law supplied a second graph using current WHO statistics.
Whether or not Mr. Law is correct remains a mystery. However, one thing is for certain: someone, somewhere, is lying. The question is: what are they covering up and why?
Conclusion: Governments Need to Stop Lying About Polio
With the lack of ethics and extortion of the poor continuing to corrupt the vaccine programs, can there ever be an end to the polio epidemic? We must ask ourselves whether or not government lies will continue to mask the facts. If the polio virus can be contracted through contaminated feces and poor sanitation, then you would expect sanitation and providing clean water to be the number one priority of governments and aid organizations.
It has been proven over and over again that vaccinations alone cannot eradicate polio. Isn’t it about time that governments stopped their lies and got their priorities right for the sake of innocent children?
See Also:
Nicholas Gonzalez, M.D. – Scientifically No Polio Vaccine was Needed
The Millions of Polio Sufferers Who Never Existed

Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?

One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.
One Comment