



Comments by Health Impact News Editor
The failure of the pertussis (whooping cough) vaccine has been well documented here at Health Impact News, as new outbreaks of whooping cough among those fully vaccinated for pertussis continues to make news.
Dr. Suzanne Humphries has been gracious enough to share her Vitamin C protocol for fighting whooping cough. If you or your child are faced with fighting whooping cough, the last thing you need is a debate on the merits of the pertussis vaccine. You need advice on effective treatment options, and that is what Dr. Humphries provides in this presentation.
See also our previous article on Dr. Humphries’ use of Vitamin C here:
Vitamin C Cures Disease but Doctors and Pharmaceutical Companies Do Not Want You to Know This
Sodium ascorbate/ Vitamin C treatment of whooping cough
I wrote the original 2012 treatment document, based on Hilary Butler’s 30 years of research and my own experience and knowledge of toxin-mediated diseases.
My motivation to find a solution came from watching two young girls that were close to me, suffer from whooping cough. Neither conventional antibiotics nor homeopathic options helped at all. A skilled and revered homeopath was so concerned, that he even said to take the antibiotics. One girl refused and the other promptly vomited up her first dose and their mother was wise enough not to push the antibiotics. I later learned that there is little to no evidence that antibiotics help the severity or duration of cough in such children.
Both of those children recovered from an illness that neither will ever forget. Their excellent baseline health and nutrition no doubt helped them survive without any huge drama. Watching them cough, made me understand why anyone ever wanted to develop a vaccine against whooping cough. The problem is, the vaccine doesn’t work well at all and has toxicity issues. Had I known about the sodium ascorbate treatment, the girls would have had a much easier time of it.
A study of the medical literature showed that there was scientific rationale for such a treatment, which motivated me start recommending vitamin C in those who have need, and to write the original document. After several years of expanded understanding of whooping cough in babies as young as 2 weeks of age, and older children, I’ve received hundreds of letters of appreciation telling me how the protocol worked for parents using it on their own.
Broader experience and observation has highlighted individual differences and unique situations, and resulted in technique refinements and improvements to the pre-existing write up. New medical literature references have also been added.
You must carefully read every word of this long document. Please do not jump to the protocol if you do not understand the full picture, you may struggle to work out how, when and why to adjust vitamin C dosing. Your child’s health and recovery is worth a few hours of your time to learn.
If you have a cooperative medical provider, this document can serve as a guideline for them and you to work together. However, as you will see by parents’ experiences on drsuzanne.net, most parents use the document on their own with success. Their stories will give you hope to put aside the negative messages propagated by ignorant and miseducated mainstream media and the conventional medical system.
B. pertussis infection as NOT a walk in the park. For many people it is a severe and worrying cough. If the B. pertussis vaccine was safe and effective, it may have been worth using. However, the B. pertussis vaccine is provably one of the most ineffective. It’s many disadvantages which lend dubious, fleeting protection to the individual, results in numerous doses and boosters from cradle to grave. In fact, the more whooping cough vaccines a person receives, the less effective they become.[1] Diavatopoulis has even compared the acellular vaccine that is used today, to allergy shots, because the cellular immune system responds less and less after successive doses in those who have been primed with acellular vaccines.
Conversely one episode of natural whooping cough renders the recovered person immune far longer than any series of vaccines will.
The information provided here is distilled from a wide body of literature that demonstrates that the ascorbate molecule, in frequent doses, is extremely safe. Experience shows it to be instrumental in the biochemical recovery from Bordetella pertussis (whooping cough) infection. Natural recovery from whooping cough has advantages for an entire life.
Bordetella pertussis infection
While it is not ideal for a newborn infant to catch whooping cough, it can be managed at home. Successful treatment will require diligence and an adult rocking very young infants, at the peak of infection, 24 hours for several days. Babies cannot get vaccinated until they are two months of age, and by then, the cough can be treated much more easily than in a younger infant. After three months, a fully breast-fed baby will respond well. Otherwise healthy babies over six months of age with whooping cough, should not worry any parent if they understand the principles and protocols to deal with the infection, and are well equipped and organized.
B.pertussis bacteria is very tricky, and part of its armor involves several toxins. Toxin production is the major reason for the worst symptoms. Conventional medical doctors don’t know how to address the toxin issue in most infections. They give antibiotics, which have never been shown with any certainty, to limit the duration or severity of whooping cough in well-established disease.
After years of experience treating infants of all ages, it has become evident that there are some exceptions to the antibiotic issue:
- In 2 week to 2 month age babies, if the antibiotic is given at the first sign of cough, the severity of cough can often be decreased. I’ve worked that out with observation and use, but the two doses of antibiotic have to be given at the very first signs of the first phase of the illness. This can only happen if the index case has previously been identified and the parents know what is coming.
- This does not seem to be the case in older babies, where parents almost always report worsening symptoms after the antibiotic has been given. This may be due to starting them after the cough is full blown. I’ve not tried the two days treatment with azithromycin on older babies, because IMO, the risk:benefit is not there at that age. One exception could be someone with cystic fibrosis or other underling lung problems. But again, it will probably only make a difference if the cough is anticipated as a result of knowing that the exposure occurred.
- Antibiotics don’t seem to help whooping cough symptoms in anyone at any age, after it has become a full blown infection.
Is ascorbate a cure? No, but the majority of parents who use it on their infected babies, and young and older children, report a significant decrease in cough intensity, with thinning and loosening of sticky mucus, within the first 24 hours of proper dosing. Ascorbate, in properly spaced, very high oral doses, will get you and your children through the weeks with vastly reduced symptoms while developing lasting immunity that will later protect those around them more effectively than vaccines can.
A 2010 study suggested that natural immunity to whooping cough lasts at least 30 years[2], whereas the immunity from a vaccine lasts three years at most.[3]
Because of the limited duration of transient immunity after vaccination, B. pertussis boosters are now being recommended for 8-12 year-olds, adults, women during each pregnancy, and contacts of newborns before every birth.
If you think that a vaccinated person cannot get whooping cough, in the most severe manner, think again. Most babies over the age of 6 months who get whooping cough are fully and “appropriately” vaccinated. In 2012, a new peer reviewed document from professor of infectious diseases, Dr. Maxwell Witt of Keyser Permanente in California showed that B. pertussis runs rampant in fully vaccinated child populations.
“Our data suggests that the current schedule of acellular pertussis vaccine doses is insufficient to prevent outbreaks of pertussis. We noted a markedly increased rate of disease from age 8 through 12 . . . . Acellular vaccines have not been studied for clinical efficacy in north America and no studies exist on long term.” [4]
Quite impressive, right? Table 1 at the end of Dr Witt’s document shows the percent of cases in the vaccinated, and it as follows: 86% age 2-7, 86% age 8-12, 62% age 13-18, 81% age 2-18. So now you know who gets more B. pertussis. It is not the unvaccinated. He even says, in the introduction:
“Our unvaccinated and under-vaccinated population did not appear to contribute significantly to the increased rate of clinical pertussis. Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group.”
The rate of infections in the vaccinated is huge. Look at this chart prepared by the California Department of Public Health, Immunization Branch.
 The above chart was last printed in the California department of public health pertussis report [5], November 10, 2011. Thereafter, the report on cases by vaccine history stopped. In fact, word searching for ‘vaccine’ brings up no data in the recent reports. It just says to give the vaccine in infancy and pregnancy.
The above chart was last printed in the California department of public health pertussis report [5], November 10, 2011. Thereafter, the report on cases by vaccine history stopped. In fact, word searching for ‘vaccine’ brings up no data in the recent reports. It just says to give the vaccine in infancy and pregnancy.
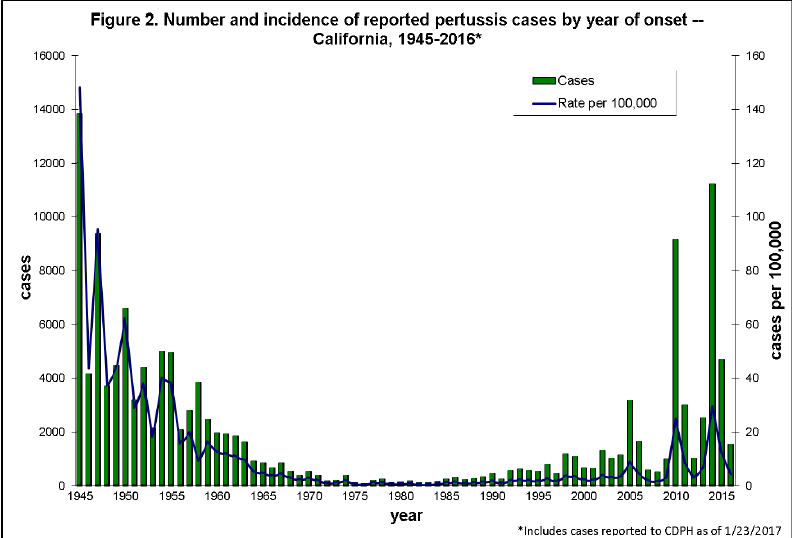
Graph – source.
Vaccine defenders will say that the high rate in the vaccinated is just because the majority of people in the population are vaccinated. There are known and published reasons why vaccinated children are becoming infected, even at high vaccine compliance rates which I have discussed elsewhere. See here:
The fact is that regardless of whether a child is vaccinated or not, everyone needs to be able and ready to treat whooping cough.
Personal protection: Who wins out?
Vaccinated babies, children, and adults are not able to mount the comprehensive bronchial and cellular immunity that a non-vaccinated person naturally develops in the course of the disease. [6] Why? Because the vaccine primes the body to fight B. pertussis toxin and sometimes a couple of other cell antigens, in the blood, but does not provide protection at the lung interface where the real life battle occurs. The ineffective immunity “learned” from the vaccine series (referred to by Dr. James Cherry as “original antigenic sin”) [7], is the same way the body will respond to a subsequent natural exposure.
The learned immune response to an acellular vaccine results in numerous differences compared with the normal response mounted to a natural infection. Some of the key differences in vaccinated people are:
- Antibody preferentially made in the blood rather than the lung interface.
- IgG antibody rather than IgA antibody.
- The wrong type of antibody because the vaccine antigens are not the same shape as the real life antigens. [8]
- A relative, progressive loss of protection with each vaccine dose, because the T cell response is similar to what allergy injections do. [9]
- Far lower complement-mediated killing of bacteria.
- Suboptimal inflammatory responses resulting in impaired lung clearance of bacteria.
- Impaired phagocytosis.
It is well known that never-vaccinated B. pertussis disease-convalesced children, develop important immune responses that the vaccinated do not [10]. The vaccinationists have attempted to compensate for this phenomenon by creating vaccines with multiple antigens. The point they miss is that it is only front line, innate, and naturally acquired complex-cellular and bronchial responses, which give the full protection. It has been shown that response to B. pertussis toxin [11] and adenylate cyclase toxin [12] is far more robust in the unvaccinated, than the vaccinated. Because of this, the naturally immune upon re-exposure, will clear bacteria far more rapidly than the vaccinated. There is an enormous difference between broad, long-lasting immunity from the normal disease, and limited antibody development and short-term pseudo-immunity from the vaccine.
If your child has whooping cough, the doctor will try to make you give antibiotics even though antibiotics do not shorten, or do anything, to lessen the course of the disease once the cough is full blown [13]. Even alternative doctors will suggest it because they don’t know the medical literature and because they want to just DO something. The conventional medical culture does not seem to understand the damage created by antibiotics.
Any antibiotics given during full-blown infection seem to uniformly make things worse. They can make the coughing fits more severe by releasing LPS(lipopolysaccharide) from other gram-negative gut bacteria during the microbial die-off that happens. This will increase the work of the liver in its detoxification of all bodily toxins during a time when lung bacteria are releasing exotoxin hand over fist. Tozzi reported that Children who received an antibiotic had a duration of cough 6 to 11 days longer and spasmodic cough 4 to 13 days longer than untreated patients. [14] The authors insinuated that the sicker patients may have been preferentially treated with antibiotics. However combining that with the Cochrane results [15] and my hands-on experience, leaves me confident that antibiotics are highly unlikely to make the established cough any better.
Convention says that antibiotics stop the recipient from coughing as much bacteria into the environment for others to catch. That is true to an extent, but I’ve seen numerous babies get the antibiotics, continue to cough, get tested again weeks later –and still culture or test positive. There is now a growing issue with antibiotic resistant B. pertussis. Azithromycin appears to be maintaining its strength against the bacteria with only one case reported in the literature of possible resistance. [16] However, I’ve seen babies treated with azithromycin continue to remain infected upon further testing.
If your child has whooping cough, you have the opportunity to control it the first time, so that you don’t have to worry about it for several more decades. Most people who are naturally convalesced and have not been given antibiotics, will not experience the cough at all later in life, because they will be experiencing a series of natural boosters in the environment, since B. pertussis bacteria appears to be continually circulating.
The whooping cough bacteria
First let it be known that the species of bacteria responsible for whooping cough, Bordetella pertussis, has properties that not all bacteria have, and that is what makes it such a problem to deal with: It secretes several toxins, and has adapted to stick to the cells of the airway.

Those parts marked “Nonciliated cells” are the damaged ones. They look like a lawn mower has cut them down.
Most of the respiratory tract lining (from the nose to the bronchi) is covered with hair-like (ciliated) epithelial cells. The cilia beat in one direction, moving mucus towards the throat where it is swallowed. Moving down the bronchi, the cells change in shape but are still ciliated. In health, the bronchial hairs are moving mucus around all the time. It is this continuous movement that keeps the airways free of invasion from pathogens. If the lungs didn’t do this, then we would not be able to get rid of the bacteria and viruses we breathe every day.
The lining mucus is part of the innate immune system and is loaded with immune globulins. So you must keep the mucus moving, especially in a sick child. Once the B. pertussis bacteria have a hold on the cilia, it secretes tracheal cytotoxin, which cuts the hairs off, stops them from beating, and destroys the cells underneath [17]. The mucus then stops moving normally and instead, it pools deeper in the lungs. Then it builds up, breathing becomes harder, and the body signals coughing to try to move the mucus out of the way, for proper breathing to occur.
As long as you keep the mucus moving, your baby should not get a secondary infection. Ascorbate and good hydration will help to keep the mucus thin. When you first start to use ascorbate, the mucus may thin out quickly and the person coughing may bring up large quantities of mucus in the first 24 hours. That is a sign of success.
There are two first-line bacterial toxins [18]; pertussis toxin (PTx) which stops the body from sending neutrophils (immune cells) to kill the bacteria, and Adenylate Cyclase Toxin (ACT). ACT inhibits the immune cell function and poisons the immune response [19], acting as a “force-field” to shield the bacteria from the immune system while the bacteria start stripping the lung cilia off of the epithelial cells. Vaccinated children cannot mount antibody to ACT[20]. Ascorbate will help neutralize these toxins while the body is mounting a proper immune response, which takes weeks.
If the disease goes out of control, toxins can enter the blood stream and irritate the body. If the baby’s immune system is not so good, or the liver detoxification system is inhibited, then B. pertussis toxins can also get to the brain, but this is very rare. This is one reason why 1 in 200 babies can die—their figures, which I am repeating back to you. What is more likely is that 1 in 200 babies who have received standard medical treatment, or no ascorbate treatment whatsoever, might die. These numbers are used to frighten parents into vaccinating, but the numbers are generated by counting children who’ve been treated conventionally, not by those of us who have successfully treated the infection in breastfeeding infants, with supportive care and ascorbate—at home. Those children rarely land up in the hospital, and thus are not counted in the stats.
If the mucus is not coughed up, other bacteria can grow and cause a secondary bacterial infection, which doctors will want to treat with antibiotics. It is believed that whooping cough can cause long-lasting lung problems, in rare cases. Yes it can, if you treat it the way conventional doctors do, doing nothing other than antibiotics. Just using antibiotics does not deal with the pooling mucus, or manage the cough, or deal with the toxins. If you keep the mucus moving, there should be no further problems other than the cough itself.
Clinical scenario and diagnosis
Whooping cough has two stages. The first stage, colonization, is like a minor cold, which can, but does not always increases in intensity over about a 10-day time frame. Then it seems like the cold is gone and there is nothing to worry about. The second or toxemic stage of B. pertussis begins gradually. The child starts the odd
cough, and after about two weeks, the cough starts to get strong, with prolonged and paroxysmal coughing that often(but not always) ends in a characteristic inspiratory gasp (whoop). The cough is often more prominent at night. If the cough changes, and becomes more of a bark, and more regular—developing a pattern at night of “every hour, on the hour”—then you have to consider that it could be whooping cough.
If you need a laboratory diagnosis, PCR (polymerase chain reaction) and bacterial culture are both available. Both have advantages and disadvantages. The culture test is less reliable than a PCR test. A negative test does not necessarily rule out B. pertussis. Blood testing is sometimes used later in the cough, but most people get their diagnosis by the more reliable PCR method. Read more about available testing on the CDC website. [21]
Most parents benefit from confirming the diagnosis. First off, you know exactly what you are dealing with, and recent contacts can be warned. Secondly, you have a record of infection that can be used as evidence of immunity later. The potential disadvantage of requesting a test is how you could be treated by the consulting doctor. It is not uncommon for parents of both vaccinated and unvaccinated children, to diagnose the cough before the doctor does, and after the doctor has misdiagnosed and misprescribed multiple times. The doctor surprisingly continues to deny parents the right to get their child tested. Often, when this happens, the parents will go to another facility and get the test, which comes back positive.
As the cough becomes more severe, various stimuli can trigger it. A classic way of diagnosis is to touch the middle of the tongue with your finger to see if this starts the cough. Or if eating (i.e., passing food over the tongue) starts a cough, consider whooping cough. If a child happens to be breathing in, as well as eating when the food touches the tongue, and the cough starts on the inhale, there is a possibility of food going down the wrong way. If this happens, you may have to do a gentle push under the diaphragm to have them pass the food back up from the trachea. Running around is another trigger.
If you watch the child, they go cough, cough, . . . cough, cough, cough, cough, cough (and at this point are starting to go pink in the face, and are starting to wonder when they can have an in-breath) cough, cough, and then right at the end, they stop coughing, and the in-breath is really fast, because they want to expand their lungs, and the result can be a “whoop.” Older children don’t whoop much, if at all.
The early progression of cough:
The cough will become more regular and predictable, first at night. You may get coughs every hour, on the hour. This is because it takes around an hour for the mucus to pool deeper inside the lungs.
Usually parents start to suspect whooping cough once the cough becomes regular in the day as well. If you suspect it is whooping cough, write down the time of each coughing spell at the beginning, to see if a pattern establishes. This will help with diagnosis.
Why write it down? Because life will become so hectic you won’t be able to remember, and your paper pad will be your memory. It will enable you to look back clearly, without panic, and see what the progression has been.
Once the cough is established, at the end of some coughs, fairly thick mucus might come up. This is because the bacterial exotoxins have eroded most of the hairs in the bronchi that normally sweep the mucus up and around, like a non-stop river to keep the surfaces moist.
The earlier in the illness you start using the ascorbate, the fewer bronchial hairs will be lost. Once bronchial hairs are lost, the cough sounds dry, and that’s because the mucus membranes aren’t being kept as regularly moist as normal. Most children do not pool mucus, so long as they continually bring it up.
Healthy babies, toddlers, and older children with whooping cough look quite normal between the telltale coughing spells.
Taking care of the caretaker
First, let’s talk about you, the parent. Most people who find this article, have first been terror-stricken by the pronouncements of gloom over their coughing child, and the huge field of fear that exists in the general public. They also may not believe that they can treat the cough without a doctor with a prescription pad, who may also chide them for not vaccinating.
If that describes you, then the first thing you need to do is take some deep breaths and think. If at first, your emotional scale is off the Richter line, that is natural—it can happen to anyone. But it doesn’t help the child. You need to stand back and analyze the situation clearly.
Get some paper and a pen. Analyze when symptoms started by thinking backwards, and writing down the progression, working up from the bottom of a piece of paper. Start writing about today, and leave spaces between each day as you write, because you would be amazed at what you remember and can fill in, as time goes by. Fill as many sheets as you can, and when you have worked out when you think exposure was, number the pages from the beginning of the infection to now, then continue on writing down exactly what you see and hear each day. (If you do need professional help, this written record becomes invaluable. Give them a copy to read.)
There are parents all around the world who know that any baby, at any age, can be managed if a mother is supported and knows what to do. A rocking chair is a must for parents and caretakers to conserve their own energy, and be able to easily rock very young babies. This will serve to keep the infant relaxed and the mucus moving.
Powdered sodium ascorbate is good for starting. You should always have this in the house to treat many different external and internal conditions. Make sure you get a non-GMO formulation. We have the most experience with Nutribiotic brand sodium ascorbate. DO NOT USE Ester-C OR Calcium Ascorbate. When using the high doses necessary for most illnesses, nobody needs that much calcium. Besides which, the intestines transport the ascorbate into the body using sodium transporters and for that reason, sodium ascorbate is more compatible biomedically.
Caretakers/parents will find whooping cough stressful. The stress can also take a toll on your health. Eat well, and if you feel you need it, you can take a large dose (one tablespoon) of cod liver oil or omega-3 fatty acid, and 5-10 grams of ascorbate spread out over waking hours. If you are coughing or under a lot of stress, it may also be a good idea to give yourself a loading dose of 5 grams in half a glass of water. If this gives you loose bowels, cut the dose back.
Mix the sodium ascorbate in whatever volume of water works best for you and split it into maybe 4 doses through the day for YOU the adult. You can also make a concentrated shot, or even dilute it much more, depending on how well you tolerate the salty feeling. Regardless of how you take the powder, you must stay hydrated with plain water all day long, especially starting in the morning when your urine is most concentrated. Hydration is important for babies too.
There is one important key for breastfeeding mothers, which I’ve seen happen numerous times, especially if you, the mother, have whooping cough. YOU need to keep your ascorbate levels consistently high all day and night, because if you don’t, your exotoxin can pass on to the baby through your milk. So, you must efficiently neutralize the toxin in your own body.
Types of ascorbate to have on hand
Sodium ascorbate crystalline from a non-GMO source. I recommend Nutribiotic brand available from amazon or iherb.
Liposomal sodium ascorbate. I recommend Livon labs brand lipospheric available from Amazon and iherb. Note that this is a soy-based product and also contains 15% alcohol and some EDTA. For non-soy sensitive children it is ideal. If the child or mother are known to be soy-sensitive, you can locate a sunflower oil based product instead.
In one child who had mild underlying kidney issues, there was some swelling with high dose sodium ascorbate. If that is an issue, ascorbic acid can be used with sodium ascorbate to cut down on the sodium. You may need professional help if swelling becomes an issue. It is very rare.
General care of the child
Watch the child carefully throughout the day, and write down everything, including how you are feeling. If the child feels hot, go ahead take the temperature. Under no circumstances use cough suppressants of any kind, or acetaminophen, fever reducers, or cold medicines. Parents have been conditioned to fear fever, but fever is the body’s innate mechanism to deal with disease.
However, know that whooping cough bacteria do not permeate into the blood and fevers are not usual in any phase of whooping cough. If the temperature is above normal, other infections should be considered. I have never seen an secondary infection in ascorbate treated children, but in conventionally treated people this can happen, most probably as a result of subclinical scurvy, white blood cell under-function, and antibiotic use which can skew the microbiome.
Let the child play at home but if they run or exert themselves, they will have a cough. Keep the child away from susceptible people, pregnant women, and siblings of very young babies until they are no longer contagious. Contagion in naturally treated children is between 3 and 6 weeks. If the cough is still roaring at 4 weeks, assume the child is still contagious, unless they’ve tested negative.
Vitamin C toxicity?
In the wake of pharmaceutical disaster after disaster in all areas of medicine, it is ironic that there is even discussion of a toxicity level for vitamin C –especially for a sick person. Vitamin C is never a poison in the body, because so many functions of the body require it, and whenever you take too much, you will have an episode of loose bowels, as the excess is removed from the body. This is how you know you’ve had more than enough.
For anyone to consider that vitamin C would have toxicity means that they have limited understanding of the various roles that it has in the body. There is a huge mass of research literature supporting the truth that vitamin C is nontoxic and safe in indicated circumstances, even in mega dose quantities. There is much evidence indicating that vitamin C metabolism changes during infections and this may change the relationship between doses and adverse effects [22] if you are burning through vitamin C. Because your body is requiring more and more, and using huge amounts of it, you will not suffer from toxicity. You will suffer if you don’t use vitamin C.
One of the biggest problems, especially in toxin-producing illnesses like B. pertussis, is that people are hesitant to use the high doses that are needed. They have been brainwashed about how dangerous ascorbate is in large doses. They see 20-30 Grams for an adult or 5 -10 grams for a child as an outrageous amount. These seemingly high doses of ascorbate are often only just enough to keep up, because the body will use it up very rapidly as it works to cope with ongoing toxin production, along with the resultant oxidative stress,. It’s like pouring water into a bucket with leaking holes. The vitamin C intake has to increase to keep up with the body’s need for it.
Nobody has ever died of a vitamin C or synthetic ascorbate overdose. The LD50 is a convention used to represent the lethal dose for 50% of a tested population. The LD50 for ascorbate is 11,900 mg/kg, for table salt 3000, acetaminophen 1944, aspirin, 200, caffeine 192 mg/kg. Think about that for a bit. Nobody would think twice before using aggressive caffeine therapy on a premature baby who had respiratory depression after a vaccine [23], or aspirin and acetaminophen for any aches pains or acetaminophen for fever. Why the concern about vitamin C/ascorbate? Ignorance.
It has been reported [24],[25] that people with serious infections can ingest over 50 g/day of vitamin C without gastric problems. This same principle whereby the use of a substance acutely needed by the body will not cause toxicity, applies to a few other nutrients during infection, like vitamin A. You can give a child with measles vitamin A in doses that would normally be considered toxic, because the action of the measles virus pulls vitamin A out of the body hand over fist. All you are doing, is replacing what the infection in the body is mining. Therefore, in the context of measles, high doses of vitamin A will not be toxic.
Kidney Stones
A healthy person doesn’t need mega doses of ascorbate when they are healthy, but only in conditions when such doses are required.
Research shows case reports of oxalate crystal formation in the kidneys of people using high dose ascorbate for various illnesses and in health, but it is very rare and can be prevented. Note that the presence of crystals in the urine does not mean stones will form. The crystals have to precipitate and join together in order to make a stone. Urine pH, citrate concentration, and other factors can control the joining together of crystal-forming elements into a stone.
Existing case reports that implicate ascorbate, do not necessarily prove ascorbate was the only factor.
People who have a condition known as primary oxalosis, are prone to form oxalate in the body. Some people who have fat malabsorption absorb more oxalate from the intestine, and those people will have an underlying risk of oxalate stones. If they ingest ascorbate, the ascorbate will usually be implicated, and in some cases it may contribute.
If kidney stones are a concern, check with your doctor. If you have a history of kidney stones, please inform yourself of the risks and be sure to drink plenty of water and alkalize the urine. I have yet to hear of or witness an infant with kidney trouble or stone formation at the time of or following ascorbate dosing. Could it happen? Yes. It is possible. But when I see an infant blue in the face and know that ascorbate will help, it seems unethical to withhold the treatment. If that same infant were septic, nobody would consider withholding antibiotics even though the chances of anaphylactic shock from antibiotics are about the same as, or higher than the chance of kidney stone formation from vitamin C in that infant. In fact, antibiotics are routinely given to B. pertussis patients despite the lack of evidence that they do anything beneficial to the recipient, once the infection is well established. I always tell parents that stone formation is a potential, but very low risk. I don’t know of any parent who has considered not using ascorbate in their coughing infants, once they learn the physiologic benefit.
If there is concern about kidney stone formation, or kidney failure, do not take vitamin C or ascorbate without consulting your doctor. In older children and adults, hydration with water and fresh lemon will alkalize and dilute the urine, making oxalate stone formation nearly impossible. If there is a known history of a stone forming disorder called hyperoxaluria, then caution should be exercised. However to be safest, keep the urine dilute and alkaline as oxalate stones form in acidic, concentrated urine.
G6PD
Anyone with a very rare disorder called Glucose 6 phosphate dehydrogenase deficiency (G6PDD), which can cause anemia and red blood cells breaking open when certain foods and drugs are given, should not use mega doses of vitamin C, except under specialist care. This issue as well as other toxicity issues are discussed in a previous BLOG[26]. If you or your family has a history of anemia or G6PD deficiency, consult a doctor well informed in vitamin C immunobiology before taking vitamin C. If I suspect there could be a family history, I always send for the blood test as early as possible. People with this disorder can still take moderate doses of ascorbate when they are very ill.
The G6PD gene is carried on the X chromosome but women and girls can still have the disease, so don’t assume it is only a male issue.[27]
How Ascorbate works
Ascorbate, being the anti-oxidant portion of whole vitamin C, is an electron donor, neutralizes toxins in the blood, and will stabilize the child. If you are breastfeeding, you will have to take it yourself and/or give it to the child until the coughing stops. It is better for you to give vitamin C directly to babies, rather than trying to guess how much is coming through breast milk. Even if you take high doses, you will not get the dose you need into the baby.
The ascorbate will not kill the bacteria, but it will mobilize the neutrophils and phagocytes (the immune cells that process the infection), which grind to a halt without it, because ascorbate is their fuel[28],[29]. The bacterial toxin forms a barrier to the immune system. In using ascorbate, you are clearing out the barrier and allowing the immune system to get in and deal with the bacteria. It could still take the whole 100 days to deal with the B. pertussis and start to regrow cilia—, but the child will have LESS serious symptoms, because you are keeping the body as clear of toxin as possible, and the immune pathways functioning properly. My experience is that most people treated with ascorbate will not cough for the full 100 days, usually 50-75 and it is a very manageable situation, with one peak week being most difficult.
The functions of vitamin C and ascorbate in any toxin-mediated disease (which includes tetanus, diphtheria, whooping cough, Staph. aureus, Strep. A, meningococcal invasive disease, pneumococcal invasive disease, etc.), are numerous. Three of the many fundamental functions of ascorbate are strengthening cellular and vascular collagen bonds, detoxifying the body, and keeping mitochondria running properly. The very common reason why people who are ill for a long time have extreme lethargy—is lack of vitamin C[30]. You can’t have functioning mitochondria without ascorbate. And it’s no fluke that if a competent doctor tests babies after SIDS, they can often find undetectable vitamin C/ascorbate levels, and bone evidence of scurvy. Okamoto has found a reproducible experimental relationship between SIDS, ascorbate deficiency, and carnitine deficiency.[31].
Here are a few functions of vitamin C, using whooping cough as the example:
- The front line function of vitamin C is to neutralize circulating toxin, which is then removed from the body before being able to destroy tissue and disrupt normal fatty acids and cell function. With whooping cough, the body manages the toxin with its antioxidant reserves, until it runs out of antioxidants. Then the toxin builds up, the cough intensifies, and there is breakthrough of toxin into the bloodstream. In babies with subclinical scurvy, the blood brain barrier can weaken significantly—and result in toxin crossing into the brain.
- When a baby with whooping cough runs low on vitamin C, the mother may notice that the child’s gums may go red around the edges—a first sign of scurvy. Then the cough gets much worse, because the neutrophils become less functional. The bacteria spreads deeper through the lungs, eroding the bronchial hairs, which means that instead of the mucus flowing up and recycling normally, it now pools at the bottom of the bronchi, and toxin rules the area. At this point, ascorbate in large enough doses lowers the toxic load, but it won’t stop the need to cough, because the hairs aren’t intact, so the child still has to cough up that pooled mucus. Ascorbate thins out the mucus, making it much easier for the child to expectorate, avoiding the blue or red-in-the-face stage, because the mucus isn’t as thick and moves up and out more easily. However, because the mucus moves up quickly, you may get the odd “vomit” session, particularly if the child has just eaten food, or swallowed the mucus instead of coughing it out. Vomiting, in my observation, seems to be a result of swallowed toxin-containing mucus in the stomach.
- Without adequate vitamin C, the integrity of the body’s collagen intracellular bonds in blood vessels and capillaries start to weaken, and the child will get pink eyes from the cranial force, the lungs can start to become congested, and the blood-brain barrier can weaken, and become permeable. Poor tissue strength will also contribute to the rare collapsed lung that the medical literature reports during whooping cough.
- Vitamin C is a prolific antioxidant. Without it, the neutrophils and liver struggle to deal with the free radicals and toxins generated by the bacteria[32].
- Vitamin C has a major role in mitochondrial function. The patient can feel exhausted without adequate reserves, because carnitine won’t pull fatty acids into the mitochondria, and thus mitochondria produce less energy.
Without ascorbate, the whole of the body’s core functions gradually shut down, and if it is not replaced, there is only one result, and that is death. You can toss everything else into a human body—every other good food or nutrient . . . but if there is no ascorbate, death will ensue.
General rules (not set in stone)
If you are using ascorbate to bond to and neutralize toxins in whooping cough or any other disease, you must use as much as the body will soak up, to get all the functions going and complete the process. Everything you put in is quickly utilized to join with exotoxin and flush it out; to keep the neutrophils moving around and dealing with waste; to keep the liver functioning well; to keep the mitochondria functioning properly; to keep the connective tissues intact; to cope with the coughing.
Powdered and lipospheric sodium ascorbate are what you have to keep in the house. It is available to you from your health food store or online from Amazon or iHerb. The lipospheric ascorbate can be used by itself in exclusively breastfed infants. Sometimes you will have to add powdered SA even to breastfed infants, when the bowels are sluggish. Anyone eating food will need powdered sodium ascorbate because it gets down to the small bowel and colon where other bacteria live which also produce endotoxin.
Some people want to use IV ascorbate, with the idea that more is better and IV is better than oral ascorbate. This is not true for most cases of whooping cough. I have had people tell me they tried IV ascorbate and it had no impact on the cough. There is a reason for that: The ascorbate, in anyone eating anything besides human milk, must get to the lower bowel to deal with everyday endotoxin production, and the pertussis exotoxin that is swallowed. If a very young infant is in the ICU with well established and severe whooping cough, before I could get to treat them at home, I would recommend the doctors give one dose of IV ascorbate plus continuing oral ascorbate or nasogastric ascorbate dosing with close monitoring of urine output and kidney function. I also would recommend administering IV hydration and continuing maternal milk either orally or through nasogastric tube. But I would never use only IV without oral dosing. So if you are tempted to go get an IV treatment for an adult or teen go ahead, but know that it is probably not necessary and that oral ascorbate has always sufficed in my infant and toddler patients.
Dealing with endotoxin in the intestine by using powdered ascorbate, spares the liver having to take on that job, which it normally does. The liver can then, more easily, deal with the other toxin being produced by the B. pertussis. Powdered sodium ascorbate is going to be necessary for any infant drinking formula and anyone who is not exclusively breastfed.
Breastfeeding moms can express some breast milk into a cup, and put a pinch of sodium ascorbate powder into it, and mix it. Then, using a plastic eyedropper, dribble this into the baby’s mouth gradually over a few minutes for each dose. Don’t squirt it in – just drip it in, bit by bit. If your baby is formula fed, that baby will require more ascorbate than a breastfed baby, and it should be dosed in the formula over the day.
Liposomal ascorbate is the same chemical but embedded into a fatty layer that does not require the transporters in the bowel for absorption. Therefore, it gets into the body differently and probably faster, using less of the body’s energy to bring it in. It is really easy to dose infants because all you have to do is take your clean finger with a dab on it and swipe it inside the cheek. Babies don’t love the taste but they tolerate it fine. Infants as young as two weeks of age have been taking it with good effect. Two week old infants usually require a whole 1000 mg sachet per day given in tiny dabs every 15-20 minutes and can require up to two sachets per day at peak of the cough.
For older children and adults, liposomal ascorbate taken just before bedtime reduces coughing at night, and can be used at the beginning of the cough, in order to boost the blood levels quickly. It can also be taken in a bolus after a severe cough.
The Protocol
The sodium ascorbate is initially dosed in a mg/kg/day fashion. Please be sure that your sodium ascorbate is a non-GMO brand. Do not use calcium ascorbate or ester-C. For babies older than 6 months, if you have to use ascorbic acid because that is all you can get in an emergency, it should be neutralized with sodium bicarbonate. I recommend you use sodium ascorbate as soon as you can get it and only use SA on infants younger than 6 months.
B. pertussis toxin excretion can be reduced to very manageable levels in 12 hours with correct ascorbate dosing. You have to continue the ascorbate for the whole time the bacteria continue to make toxin, which can be up to three months. Ascorbate does not prevent or stop the disease. It helps clear away the toxins, and makes the coughing much, much milder, increases the ability of the body to clear out the bacteria and develop immunity naturally, and vastly reduces complications.
The starting dose in children for sodium ascorbate is 200-375 mg per kg over 24 hours. But at peak of coughing, the dose needed in toddlers and older children can be as high as 1000 mg/kg/day.
If they are coughing until they are purple, or gasping, then your doses are much too small or infrequent. Bump them right up to the level of 375 milligrams per kilo of body weight over the waking hours, as a starting dose and know that you may still need much more.
If you use pounds, know that one kilo is equal to 2.2 pounds. So get a calculator and weigh your child and convert their weight to kg.
Lypo SA (LSA) or Powder SA (PSA)?
Parents want to know how to decide which to give. Generally, non-exclusively breast feeding babies and older people will need PSA and you dose it more frequently the younger the infant or child is. You start with the PSA in frequent doses because the more frequent you dose, the more the body and colon will tolerate. Once you get intestinal gurgling, smelly gas, or loose bowels you’ve got to the bowel intolerance level and probably hit the maximum dose and frequency that will be tolerated. If severe coughing is still happening, then you will have to add on some LSA.
The flush: Diarrhea after a certain amount of PSA, is commonly called the bowel flush. My goal is minimum of two loose bowel movements in infants, children, and adults. Breastfed infants will often move bowels more often than twice, so those babies don’t need any push to make more stool. Anyone who is not having at least two loose (not necessarily watery) stools per day needs more PSA. If an older child or adult develops diarrhea, you will probably notice the cough is better just after that flush. That is not a bad thing but you don’t want anyone having ongoing diarrhea or becoming dehydrated. If a flush happens, then either cut back the PSA dose or give in smaller doses more frequently. You may have to switch over to LSA if the diarrhea is not stopping after one flush.
Liposomal ascorbate can be used by itself in exclusively breastfed infants. Sometimes you will need to add powdered SA. Liposomal can be used alongside powdered SA in someone who is already taking powdered SA, yet still needs more ascorbate, but has hit bowel intolerance with the SA. Liposomal does not cause diarrhea except when taken in very high doses.
Exclusively breastfeeding infants can usually be dosed with only LSA. If for some strange reason they get constipated and are still coughing, then give some PSA in small pinches in expressed breast milk administered with a dropper.
Don’t rely on any vitamin C you take to get to your child through your milk. It takes about 8 hours for the vitamin C the mother ingests, to get through to the breast milk, and if your infant’s ascorbate needs are high, you don’t want that gap. If your own need increases, even less will get through into your breast milk.
NEVER DOSE A SLEEPING BABY OR CHILD. THEY CAN BREATHE IN THE ASCORBATE WHICH CAN LEAD TO BIG PROBLEMS. IF YOU THINK A DOSE NEEDS TO BE GIVEN, WAKE THE BABY UP.
Dosing
Here is how you arrive at the amount of milligrams of sodium ascorbate, which will be spread out over 24 hours, in multiple doses. You will have to split up the baby or children’s doses in small amounts of water or human milk through the day, and because they are small they need it concentrated. You must however make sure to keep everyone well hydrated with human milk or water all day, and if you are breastfeeding, you need to be very well hydrated to pass that water on to the baby. We don’t recommend giving water to a breastfeeding baby whose mother is producing well, but rather to just feed mother’s milk as much as possible. You want to see really wet nappies/diapers.
Sometimes babies get whooping cough just after being introduced to food. In that case I recommend you stop the food and go back to all breast milk whenever possible. The reasons being that exclusively breastfed babies tolerate the cough way better than formula fed or babies already on food. In addition, aspiration during a cough could be a problem with food.
The following dose is just a guideline to start working with. You may determine that you require more or less. This is explained below.
If using pounds, use this equation: (weight in pounds divided by 2.2) times 375 = the 24 hour dose, in mg per kg.
Example: If your child weighs 20 pounds then you have 20 divided by 2.2 times 375= 3409 mg of vitamin C/ascorbate powder to be given in a 24-hour period in many small divided doses.
If using kg, just use wt. in kg times 375= your dose of sodium ascorbate for 24 hours in mg per kg to be divided into many doses over 24 hours.
Keep a chart on the fridge so that you can see what you have done, and also write down anything that tells you you have reached bowel intolerance, or any fact you feel is relevant and might need checking later.
If the patient consumes more than you calculate before the 24 hours, and there was no bowel intolerance, it was obviously needed. Do not worry. If the child needs higher doses, just give them. Most parents are concerned about giving too much and can be reluctant to dose high enough. Just make sure they are staying hydrated and the diapers are as wet or wetter than normal.
A pinch of ascorbate is about 250 mg. If you want to be more exact about dosing, calculate the amount you estimate will be needed in 24 hours, put the powder into a little container and just use pinches in expressed breast milk through the day and night.
For older children with higher doses, calculate the daily dose and give it hourly or as often as needed in divided quantities.
If using liposomal ascorbate on infants, you will need to dose every 15 minutes to every hour. If there is a big cough, you will need to give a bigger finger swab into the cheek and increase the dose or frequency.
Two to four week infants usually require 1-2 sachets of lipospheric ascorbate per 24 hours. Five to eight week babies usually require 1-3 packs. Treating such very young infants usually requires assistance from a medical practitioner and very close monitoring, often rocking the baby all day and night during the peak days.
If you are having any trouble or doubt on the dose, please check with someone who can do this calculation for you. Once you start using ascorbate, the mucus will thin out considerably. The first 24 hours may be a time when mucus seems to come out in great abundance, as it thins.
If your dose is right, within 8 hours there should be a significant reduction in the coughing frequency and severity. If you start to taper the ascorbate too soon, e.g., before two-four weeks, you could see an increase in cough. You will then have to increase the doses back up to the old dose. It is probably not a good idea to even try stopping before 4 weeks.
If your child develops very loose bowels, then you may be giving too much. In this case cut back by 50% and monitor. Bowel intolerance will also tell you when it is time to taper. Eg. The cough will be less intense and the bowels will not tolerate as much ascorbate. Start slowly tapering. If the cough worsens then just go back up to a higher dose in order to control the cough.
Note: going back to school or daycare will require an increase in dosing in the day as anything happening outside the home increases stress, even if they are having fun. Send the child to school with water containing PSA or with a few sachets of LSA to have in case coughing increases while away from the home.
The cough in most children will decrease to at least a quarter the intensity it was, after proper doses of ascorbate are given. But you still have to know how to manage the quantity of mucus that even well managed whooping cough produces, especially in babies. The babies’ relative inability to use the stomach muscles to cough properly and their narrow bronchi put them at a physical disadvantage compared with older children. If that mucus is not shifted, then secondary bacterial infections can set in, which can cause new problems. I have yet to deal with a secondary infection in all the hundreds of cases we’ve personally dealt with.
Oxygen saturation can drop in any infant during the cough, and it is usually not a problem, and not even diagnosed. However, in someone who lives at high altitude, and has underlying lung issues, or any pre-existing comorbidities, it can be troublesome. In that case, outside help could be needed and even a portable oxygen tank for low flow oxygen.
If you are giving a high dose and it seems to not be working, there may be reasons why.
Some confounding issues and how to deal with them:
- Sugar in the diet. This includes honey, rice, carbs, and all good sugar. Sugar competes with the vit C transporter in cells. Limit it. If the cough is still bad, limit all sugars even more.
- Pasteurized milk should be absolutely avoided. Some older children can tolerate fresh raw milk, but if it worsens the cough, you have to stop it. Lactating mothers can drink fresh raw milk but if you notice the cough worsens in the baby, then you have to stop it. Butter, eggs, and hard cheeses are all good for mothers and most children.
- Most vegan mothers go onto butter and eggs at my request during the infant treatment period. I also ask them to have some bone broth but most of them cringe at the idea.
- Consider avoiding wheat and gluten for a few weeks, especially if you or the child have any known sensitivities.
- Pedialyte or any sucralose-containing products are poisonous and immune suppressing. Avoid them. If you are concerned about dehydration or electrolyte imbalance then use water or coconut water in older babies and children. Fresh organic coconut water is so much like human plasma it has actually been given IV in emergency war times with success. Coconut water is not the same as coconut milk, so don’t use coconut milk for hydration. Human milk is always preferred when available.
- If a lactating mother’s milk is drying up, it can often be increased with more suckling and putting the baby to the breast as much as possible. Another successful intervention to increase milk production is a homemade drink known generically as “tiger’s milk”. Google the recipes. The key nutrients which increase milk production contain inositol and B vitamins. Also eat foods with inositol.
Managing the cough in young babies
With any cough, particularly whooping cough, turn the baby around, with its back to your abdomen. While sitting down, split your legs, so the baby is supported around the abdomen but the legs are straight down between your thighs. Your hands make a gentle net around the baby’s ribcage and abdomen, and when the baby coughs, you lean forward slightly to angle the baby, allowing the baby to have something for the abdominal muscles to push against as it coughs. You give the baby some pressure to use, but do not press in yourself. They haven’t learned to control their muscles to get an efficient cough yet, so your hands give them a wall to push against, and make it much easier for them. You may get a clear mucous glob ejected onto your floor. Better out than in. Don’t attempt to catch it, or you may drop the baby.
Some parents like to put the baby on the shoulder and bounce and rock. Some dads put them on the forearm. You have to find the position that works best for you and the baby. These are all just suggestions.
If your child’s cough is whooping cough, it may last the normal time—supposedly 100 days, but the cough will be a nuisance only, after the 5-7 day peak period.
With young children, eating can sometimes provoke a coughing fit. Know that, and give a child a small portion first. If that triggers a coughing fit, sometimes they will also vomit up what they have just eaten, particularly if they have swallowed mucus after coughing. After they have coughed and/or vomited, they will usually be able to eat again without coughing or vomiting.
If you are breastfeeding, you may notice that each time you feed, this could provoke a cough, usually during a brisk “let-down.” Deal with the cough first—let the milk spray if need be. Get the mucus up from the baby’s stomach, then put the baby back on the breast straight away. If you do it that way, there should be no cough because the mucus has gone, and baby will take the full feed. It is best to get that toxic mucus out of the baby BEFORE the full feed. This could require you putting the baby to the breast and taking them off after a 30 second to a minute, letting them vomit, and then restarting. It depends on whether they are vomiting or not. The aim is to get the vomit up before the full feed. The same process applies to formula fed babies.
Babies with whooping cough sleep lightly. An experienced mother who has gotten several babies through whooping cough said this:
I organised the house so that I sleep with the babies in a huge double bed (on the floor, not raised) and during the day, apart from toilet stops, well planned… I spent most of the day in the rocking chair if the baby was asleep, or put them in the back-pack if I needed to do a job, though I got a couple of well-placed mucus globs down the back of my neck. Everything was organized so that I got the maximum sleep, as sleep deprivation for the mother is the main problem. Littlies seem to be forever bounding with energy, even though they are coughing – somehow they cope with sleep in short burst better than we do. Cleaning – went out the window – I concentrated on cooking, dishes, and keeping up with the washing. A bath or shower was when hubby was at home, and on hand to help – to do baby as well.
WARNING: If you stop the ascorbate too soon, you will quickly find that the cough becomes much stronger. Once kids know that it’s the ascorbate that holds the cough intensity down, and parents stop it too soon, the kids will come back and plead for it. It needs to be used for several weeks, or else you will have a continuous relapsing and seeming recovery cycle. A properly-managed baby or child with whooping cough should not lose any weight at all when coughing and food intake is managed properly. Though, once in a while there is a very small weight loss which will be rapidly regained plus more immediately after recovery.
The post-recovery period
If your child gets a cold within 6-9 months after having recovered from whooping cough, the child may start to “whoop,” or cough, the same way as when processing the B. pertussis. The reason for that is that it takes time for the lung hairs to grow back. Any infection without proper ciliary motion, will result in mucus pooling. Because there has been loss of the hairs in the bronchi, this mucus pooling is necessary to trigger a cough strong enough to get the mucus from the bottom of the bronchi up to the top. Do not use cough suppressants because you could end up with pneumonia.
Some babies finish the cough and are transitioned onto regular food shortly thereafter. Note that this could cause a transient higher need for ascorbate.
Read the full article at drsuzanne.net.
Comment on this article at HealthImpactNews.com.
Sodium Ascorbate Treatment of Whooping Cough PDF down load HERE
Abbreviations:
SA sodium ascorbate
AA ascorbic acid
LSA liposomal/lipospheric sodium ascorbate
PSA powdered sodium ascorbate
WC Whooping cough
References
[1] Diavatopoulos 2017, What Is Wrong with Pertussis Vaccine Immunity?, PMID: 28289059
[2] Wearing, HJ, Rohani P.2009. “Estimating the Duration of Pertussis Immunity Using Epidemiological Signatures.” PLoS Pathog. Oct;5(10). PMID 19876392
[3] Feunou 2010, Long-term immunity against Pertussis induced by a single nasal administration of live attenuated Pertussis BPZE1, PMID:20708998
[4] Witt et.al, 2012. “Unexpectedly Limited Durability of Immunity Following Acellular Pertussis Vaccination in Pre-Adolescents in a North American Outbreak.” Clin Infect Dis. 2012 Jun;54(12):1730-5. Epub 2012 Mar 15.
[5]https://archive.cdph.ca.gov/programs/immunize/Pages/PertussisSummaryReports.aspx
[6] Mills K.,2001. “Immunity to Bordetella Pertussis.” Microbes and Infection, (3)655−677 PMID: 11445452
[7] Cherry AD., 2004 “Determination of Serum Antibody to Bordetella Pertussis Adenylate Cyclase Toxin in Vaccinated and Unvaccinated Children and in Children and Adults with Pertussis.” Clin Infect Dis. Feb 15;38(4):502-7
[8] Eberhardt 2017, “What’s wrong with Pertussis vaccine immunity?”, PMID: 28289058
[9] Ibid Diavatopoulos 2017 PMID: 28289059
[10] Cherry JD et. al., 2004. “Determination of Serum Antibody to Bordetella Pertussis Adenylate Cyclase Toxin in Vaccinated and Unvaccinated Children and in Children and Adults with Pertussis.” Clin Infect Dis. Feb 15;38(4):502-7 PMID 14765342
[11] Cherry JD et. al., 2010. “Antibody response patterns to Bordetella Pertussis antigens in vaccinated and unvaccinated young children with Pertussis.”Clin. Vac. Immun. May 17(5): 741-747. PMID 20335431
[12] Ibid Cherry 2004
[13] Altunaiji S et al.,2007.”Antibiotics for whooping cough.”Cochrane Database Syst Rev. Jul 18;(3) PMID 17636756
[14] Tozzi et. al, 2012. “Clinical Presentation of Pertussis in Unvaccinated and Vaccinated Children in the First Six Years of Life.” PMID: 14595048
[15] Ibid Altunaiji 2007.
[16] Guillot et al, 2012. “Macrolide-Resistant Bordetella Pertussis Infection in Newborn Girl, France”. PMID 22608348
[17] Cookson, BT.,1989. “Primary structure of the peptidoglycan-derived tracheal cytotoxin of Bordetella Pertussis.” Biochemistry.Feb 21;28(4):1744-9 PMID 2541765
[18] Carbonetti NH et al., 2005. “Pertussis Toxin and Adenylate Cyclase Toxin Provide a One-Two Punch for Establishment of Bordetella Pertussis Infection of the Respiratory Tract.” Infect Immun. 2005 May;73(5):2698-703 PMID 15845471
[19] Goodwin MS. 1990. “Adenylate Cyclase Toxin Is Critical for Colonization and Pertussis Toxin Is Critical for Lethal Infection by Bordetella Pertussis in Infant Mice.” Infect Immun. 1990 Oct;58(10):3445-7. PMID 2401570.
[20] Ibid Goodwin
[21] CDC last accessed August 24, 2017 https://www.cdc.gov/pertussis/clinical/diagnostictesting/diagnosis-confirmation.html
[22] Harri Hemilä. 2006. “Safety of Vitamin C: Urban Legends”, Department of Public Health, University of Helsinki, Helsinki, Finland.
[23] DeMeo 2015, Adverse Events After Routing Immunization of Extremely Low-Birth-Weight Infants. JAMA Pediatrics, PMID:26030302
[24] Luberoff BJ (1978) Symptomectomy with vitamin C: a chat with Robert Cathcart, MD. CHEMTECH 8:76-86
[25] Cathcart 1985, Vitamin C: The Nontoxic, Nonrate-Limited, Antioxidant Free Radical Scavenger, Medical Hypotheses 18: 61-77.
[26] Humphries, Suzanne, Aug 3, 2012, “Why is nobody studying vitamin C in whooping cough?” http://www.vaccinationcouncil.org/2012/08/03/why-is-nobody-studying-vitamin-c-in-whooping-cough-by-suzanne-humphries-md/
[27] G6PDdeficiency.org http://g6pddeficiency.org/wp/g6pd-deficiency-home/women-with-g6pd-deficiency/#.WaiJYIpLdE4
[28] Bozonet et.al 2015, Enhanced Human Neutrophil Vitamin C Status, Chemotaxis and Oxidant Generation Following Dietary Supplementation with Vitamin C-Rich SunGold Kiwifruit, Nutrients, PMID:25912037
[29] Schorah 1996 Total vitamin C, ascorbic acid, and dehydroascorbic acid concentrations in plasma of critically ill patients.PMID:8615361
[30] Sagun KC et al.2005. “Vitamin C enters mitochondria via facilitative glucose transporter 1 (Glut1) and confers mitochondrial protection against oxidative injury.” FASEB J. Oct;19(12):1657-67 PMID 16195374.
[31] Okamoto M. 2005. “Is sudden death with vitamin C deficiency caused by lack of carnitine?” J Clin Forensic Med. Jan;13(1):26-9 PMID 16084747
[32] Chatterjee et al. 2008. “Ascorbate sustains neutrophil NOS expression, catalysis, and oxidative burst.” Free Radic Biol Med. Oct 15;45(8):1084-93. PMID 18675339

Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.