Comments by Brian Shilhavy
Editor, Health Impact News
In our recently published article on Sudden Infant Death Syndrome (SIDS) we referenced how the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) list 130 official ways for an infant to die according to official categories of death, but adverse reactions to vaccines is not one of them.
Joy Fritz is a Death Certificate Clerk, and she recently published some of her observations in the field of death recording on Facebook.
Joy relates how she and her husband were concerned about the severity of the flu season as was being reported in the media, and that she “started reading the FDA package inserts for different flu immunization options to get informed on which immunizations might be safest for our <1 year old and 6 year old.”
She states that she wanted to make an informed decision for her family, and that
“What I ultimately wanted to compare was the risk of death.”
She learned that public records on influenza deaths stated that there were no deaths related to adverse reactions to flu medications or flu shots.
However, being in the field of death recording, she dug deeper, and has presented her research and experience to the public.
She writes:
Our current system for capturing mortality rates can and does provide a mostly uninvestigated and inaccurate picture of what causes a death. The process for creating and registering causes of death for public records is a complicated, convoluted, politicized, completely open to both ignorance and the manipulations of personal, professional, and governmental interests.
I’m the one creating these statistics and I offer you this: If you take one thing away from this, take away a healthier skepticism about even the most excepted mainstream, nationally reported, CDC or other ‘scientific’ statistics.
I am thankful that Joy reached out to us here at Health Impact News and encouraged us to share her perspective to our readership.
A Humbling Exposé into the Creation of Mortality Rates and its Impact on Our Public Health Beliefs and Choices
I work with doctors, coroners and the local county registrars everyday to create death records. It’s what I do for a living and wanted to share my thoughts on the mortality rates being thrown around on main stream and social media regarding the influenza epidemic. Please note: This information I am sharing is not limited to influenza reporting, but rather, serves as a case study of how the mortality rate recording system (mal)functions at large.
I am sorry to say that death rates are NOT as simple nor as valid as every news broadcaster with perfectly-trained vocal delivery makes them sound, and they are absolutely not the infallible pillar of medical history as the CDC purports.
Our current system for capturing mortality rates can and does provide a mostly uninvestigated and inaccurate picture of what causes a death. The process for creating and registering causes of death for public records is a complicated, convoluted, politicized, completely open to both ignorance and the manipulations of personal, professional, and governmental interests.
I have come to realize how greatly this reality becomes a public health issue during this past flu season when every major media outlet is providing us with live updates on the accruing death toll. Seeing these reports caused me concern for my family.
My husband and I discussed what preventative treatment we might consider. I started reading the FDA package inserts for different flu immunization options to get informed on which immunizations might be safest for our <1 year old and 6 year old. What I ultimately wanted to compare was the risk of death.
My kids getting sick is just part of life, other people getting sick is just part of life, lowering the risk of death to my family and the people around me is what I cared about when it came specifically to the seasonal flu.
I started researching mortality rates to find the line item in the CDC reports for deaths due to influenza vs adverse reaction to influenza medications and immunizations.
I found influenza rates, no problem.
Flu medications and shots? No deaths reported. Awesome. What a simple decision to make.
But, being in the mortuary industry and curious how they get these reports, I looked at the last full report for 2014 and dug deeper and found that they simply code and reorganize the data that they receive from death records. The death records that I am typing up and registering everyday.
So my head started exploding. And I felt, and still feel, sick. I have realized that without knowing it, I knew exactly how influenza deaths are recorded, and I know exactly why there is no line item in the CDC’s mortality rates for adverse reactions to common medical treatments.
Before I continue, please know that I will not be explaining all the ins and outs of my job, nor the incredibly rare reality that medication complications and adverse reactions do get captured (usually in box 112 of the death record, not as the primary underlying cause).
Those exceptions are made possible by exceptional, and likely, very principled people, choosing individually to go above and beyond the call of protocol, whether that be the family that is aware of the impact of the legal documentation that occurs after death and stays level-headed and involved mere hours after the death of their loved one, or an insanely humble and honest doctor, in conjunction with the coroner medical-legal officer that trusts and cooperates with the honest doctor and vigilant family to think outside the box of their standard procedures.
Almost 5 years and nearly 5,000 death certificates later, I can say with confidence that that kind of post-death communication concoction is at a statistical percentage point that even the CDC would consider insignificant.
So, in the spirit of very uncomfortable truthfulness I will share a snapshot of the core issues embedded in the daily procedures of creating the death statistics that we so desperately need to make prudent health decisions for ourselves and our families. I will also include some examples of how these core issues would manifest into faulty statistical analysis at the level of our public health and lead to the miscalculation of the benefits and risks surrounding our individual medical choices.
Core Issue A: Doctors that provide causes have not all been trained the same way, and therefore do not provide standardized responses.
This may at first glance seem minor, as it always has to me, but this directly affects the cause that the doctor lists on the death certificate.
Some doctors prefer providing the underlying cause of death as something that has happened immediately in the last days or weeks before death such as pneumonia or influenza, and leave out the more chronic illnesses. Other doctors decide they will provide the more long-standing health conditions as the cause of death such as diabetes, asthma and congenital abnormality while leaving out the more immediate illnesses.
Some doctors include both the short term and long term diagnoses. This has to do with many factors such as in what capacity the doctor saw the patient -hospital vs hospice care for example- or the immediate availability of the complete medical record within the time frame being impressed by the mortuary due to upcoming funeral or cremation services. Or, simply due to the way the doctor personally prioritizes information.
Again, way too many factors to go into here, but the basic issue of the lack of standardization in cause of death diagnosis and reporting remains.
In this case the same patient can have all these conditions: influenza, pneumonia, diabetes, asthma and congenital abnormality on his/her medical record simultaneously and any one of those conditions listed are correct and valid and could be entered as a stand alone cause and be registered by me and the local and state registrars offices without a query.
It’s the doctor’s preference and his medical opinion – yet the national attention given, medical research dollars, and yearly health choices we all make are swayed by which ever cause this particular doctor, with his/her own particular training and personality decides to jot down on the worksheet and send back to me to enter into the official record.
CORE ISSUE B: What most people don’t know is that doctors are not allowed to attest to anything that is not a strictly NATURAL cause of death.
Falls, medication complications or overdoses, causes with the word ‘injury’ in it, anything that is considered an unnatural or external cause is outside the realm of their jurisdiction as far as the death record is concerned.
The Coroner would need to be contacted and agree to certify or co-certify a death record that has an unnatural or external cause listed.
This is a whole other, very complicated reporting issue that I will not get into in this post.
I will say, however, from perspective of a mortuary representative, that everyone involved (doctor, coroner, registrar and myself) understands that the delay caused by any coroner involvement is highly dreaded and avoided if at all possible due to the amplified grief it can cause the family if they do not want an autopsy or investigation done or have to suffer a delay in services and or an upset in their own personal closure process.
However, the majority of doctors are aware of their own limitation to certify only natural causes of death. And usually in the interest of serving the grieving family, will provide the simplest natural cause that they know will quickly pass the approval of the local registrar’s office, fulfill their duty as a signing physician, and enable the grieving family to move forward with their scheduled burial or cremation services.
It should be noted here that doctors are under an additional pressure since they have a limited time set out by their State Health and Safety Codes to provide causes of death to a funeral home.
In California it is within 15 hours of death, although that is rarely achieved. Delays of more than a few days after death would risk them getting their license reported to the the state medical board for lack of compliance.
What works about this system? The system is created in such a way that naturally occurring infectious disease (such as influenza) CAN and is being reported and recorded in national mortality rates. However, the lack of standardization in the way doctors report it creates an unreliable number to set as the threshold for what constitutes an epidemic.
What does NOT work about this system? It does not report on the true consequential timeline of the patient’s medical treatment, including unnatural and external complications and errors in their medical care and is therefore woefully inadequate to make ANY medical claims or recommendations.
The first example to illustrate the impact of this issue is as follows:
I read a post from a nurse the other day that shared her story of being hospitalized due to complications of the flu. Even though she had gotten the flu shot every year, she had only gotten influenza this year. Five days after experiencing flu symptoms she went into her medical provider and was prescribed Tamiflu.
She went through her course of medication. Her flu symptoms eased but she started getting a tightness in the chest, which further worsened until she needed to be hospitalized for pneumonia and a close call with sepsis.
The conclusion of her post -and her medical opinion as a nurse – was that this year’s flu was very dangerous and anyone less healthy than her could have easily died with her symptoms, so she urged everyone to please get the flu shot to prevent the flu from spreading.
The saddest part about reading her story was discovering that she must not have read the Tamiflu manufacturer’s insert, which states that:
“No influenza vaccine interaction study has been conducted” and “Efficacy of TAMIFLU in patients who begin treatment after 40 hours of symptoms has not been established” and furthermore, “Events reported more frequently in subjects receiving TAMIFLU compared to subjects receiving placebo in prophylaxis studies, and more commonly than in treatment studies, were aches and pains, rhinorrhea, dyspepsia and upper respiratory tract infections.”(emphasis added)
This would lead to an alternate, very feasible medical conclusion that her hospitalization and pneumonia was the result of using a medication that has not been tested on a population of her vaccination status and symptoms duration, which also has the adverse reaction of a URTI.
But what if it wasn’t her? What if someone less healthy than herself with her exact symptoms and medication course HAD died?
Her medical opinion, and many other medical care providers opinion would have been that it was influenza that had caused the death, instead of the complications of the medication.
In the medical provider’s mind, the likelihood of influenza causing the death is greater than the medication causing the death because of mortality rates – but they are the ones creating the mortality rates – so what is considered reasonable likelihood is being created in a closed loop. A regurgitating cycle.
So, whether the attending physician at the hospital was aware of this medical misstep by the other medical provider or not, in this case the hospital physician could simply put ‘Influenza’ on the causes of death worksheet and send it back to me. Influenza would be entered in the death record and be reported in the state and then national database as such with no question from me or the government registrars.
What this has created, then, is a serious public health reporting conundrum. Death due to complications of improperly prescribed medication are NOT being calculated into the national reporting agencies in a real-time setting.
Neither would they be communicated in real-time to the public. Instead the public would simply hear of the rising influenza death toll and run for more medication (and likely not be reading the manufacturer’s insert either to verify if they truly are a good candidate for that medication).
In this medication example, as you can imagine, even IF they realize that the medication was prescribed erroneously, it would not be in the professional best interest of the medical provider or medical facility to report this prescription error and it’s possibly fatal complications to the family or public health officials.
I have many friends and family in the medical industry and it is easily admitted that legal and personal liability is a factor in the considerations of proper reporting.
However, if and when this possibly fatal prescription misstep was ever reported it would be in some very passive EMR analysis many months or years later, with no urgency or real-time public health warning. The ability for government to cross-check and minutely examine nearly 3 million decedent medical records of varying electronic availability – annually – it’s just not there.
This failed mechanism in the mortality rate ‘generator,’ if you will, is the same for the hotly debated adverse vaccine reactions. This is the reason you see horrible adverse vaccine reactions and deaths being claimed by parents on social media, but no item line for them in national statistics.
It is not because they don’t exist or don’t happen. The real-time data reporting system of death recording is not set up to calculate these deaths.
For the families that become aware of the adverse reactions in time to request investigation (<24 hours after death), and are able to request any relevant pathological specimens to be procured before the burial or cremation of their loved one, would then need to have the time and resources to go through the lengthy reporting and court procedures through VAERS.
A very few families do, and if they can establish enough scientific evidence (like pathology reports), find and produce enough experts and professional support, they MIGHT eventually get the causes of death amended and compensation for their loss paid out by the allotted government fund. And after 5, 10, 15 or 20 years, this passive data capture system might accrue enough statistical information to be reported back to the medical community so that they adjust their recommendations.
So, just like in the medication example, any death due to an adverse reaction to the flu shot or for ANY regularly scheduled wellness immunization, would similarly not be captured in the standard process of death recording.
As before, the doctor can still provide either influenza or any other natural occurring immune response as the only cause of death. He would send it to me and I would enter it in, get the state to approve it, and ‘Viola!’ – a thoroughly inaccurate mortality rate reporting.
In Conclusion
One of the most difficult realities for me to recognize in examining the mortality rate reporting system that I am a part of, is that the medical community itself is suffering from the ignorance that this kind of circular mortality rate generating system creates. Doctors and coroners are limited by the already existing mortality rates to gauge the likelihood of what caused death.
That kind of system can only regurgitate the same causes of death over and over again by forcing its reporters to use the same types of ‘acceptable’ death diagnoses as what ALREADY exists.
And these are the statistics the medical community uses to educate themselves and provide informed consent to the patient on what the most prudent option is for medical care to safeguard health and prevent death.
And, yes, I will take the opportunity here to say that we can logically apply this critical analysis of the lack of proper data capture to those reluctant to vaccinate or use medications.
There is no current national data capture system that records the morbidity or mortality rates of those who chose less medical intervention or choose to not vaccinate themselves or their kids. We don’t know what their life expectancy, quality of life or mortality rate is in our modern day, with the advancements in hygiene, technology and post-disease-diagnosis medical care availability being considered. It could absolutely be worse, statistically, but we wouldn’t know.
For nationally reported statistics we are left then with bad data on one side, and no control group data on the other. Hardly the recipe for safe or settled scientifically guided medical care.
Now where does that leave you and me? Our highly subjective yet somehow infallible weaponry of mortality rates – whether from national statistics or the social media horror stories – has us and all our friends and family swinging the manic flag of ‘People are dying!’
This flu season for example, some of our friends are saying ‘People are dying from flu! Get vaccinated! Take medication!’ or other friends are saying ‘People are dying from adverse reactions to medications/shots! Don’t get vaccinated! Drink elderberry!’
And we are all running for the nearest remedies that we are sure will help us – why? Because of statistics – OR because we don’t see statistics reflecting our lived reality, so we do the best we can to discern our health without statistics.
But I’m the one creating these statistics and I offer you this: If you take one thing away from this, take away a healthier skepticism about even the most accepted mainstream, nationally reported, CDC or other ‘scientific’ statistics.
Humans who had no concept of their national impact made them. The numbers are not hard – they are very, very fluid. And conversely, have a healthier skepticism about all the alternative remedies we welcome as hopeful scientific-ish options. There is no unbiased, century long, data capture system set up for these choices either.
As a parent, the most painful part of taking a step back and looking at all this, is having to humbly admit – I don’t know what the right thing to do is.
I don’t have the unbiased data I need to make the safest decision for my children.
I don’t know what the right thing to do is for myself, or for my husband.
I don’t know what side of the fence to stand on in the vaccination and mainstream medicine battlefield, and I don’t want to stand on a side: I just want the unbiased, uncorrupted and standardized data needed to accurately assess the benefits vs. the ultimate risks for my family’s health.
In the face of this fallible data capture system, my own resolution that I am willing to publicly recommend – no matter what medical choices you decide is best – would be for us all to become self reporters. Keep a health journal for each family member complete with dates and times and severity of symptoms of illness and track dates and dosages of any medical treatment administered.
Track degree of fevers, severity of migraines, frequency of ear infections, changes of behavior, hospitalizations, medications dosages and immunization combinations etc.
Think critically and ask questions when you see inconsistencies in any health recommendations offered to you or your family. Request and encourage a satisfactory discussion of benefits and risks with your medical provider.
Download and thoroughly read the manufacturers insert provided on the FDA’s website for any medication or immunization you are considering and verify that you are a good candidate for that medication.
If you decide to use that medical treatment, record any minor reactions in the health journal and immediately report any somewhat severe reactions to your medical provider and ask for that information to be added to your electronic medical record so that it might inform any future medical provider on your individual contraindications you may have in other medication courses.
Remember that each of us is liable for our own health choices, you cannot expect a medical provider to be a perfect assessor of what’s best for you.
Follow up and make sure proper reporting was done on the medical provider’s part to the appropriate national databases, or report it yourself.
MedWatch reports for medications and VAERS reports for vaccines.
This recommendation is less for you and more for others and for the sake of having the appropriate authorities informed so they can eventually take medical treatments off the market and create the demand for safer ones.
Those kind of databases can only function well for the populations they serve if they are being used by everyone.
My Final Thought: Yes, people are dying. Everyday. I do their death records every flu season or surfing season.
And try as hard as we do – and no matter how absolutely shredded inside I am especially when I do an infant or child’s death certificate- we will never eradicate death.
We CAN work to slowly eradicate and reform bad systems and misinformation. And even though there is no immediate gratification in it, we will probably save more lives when we work intelligently, truthfully and ethically towards a better future. And that usually starts with a lot of humility and admitting that change is needed.
If anyone has ideas, would like to share their thoughts or their own expertise for consideration, or somehow otherwise contribute to unifying this polarized health battlefield, feel free to add a comment.
Comment on this article at HealthImpactNews.com.
Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?
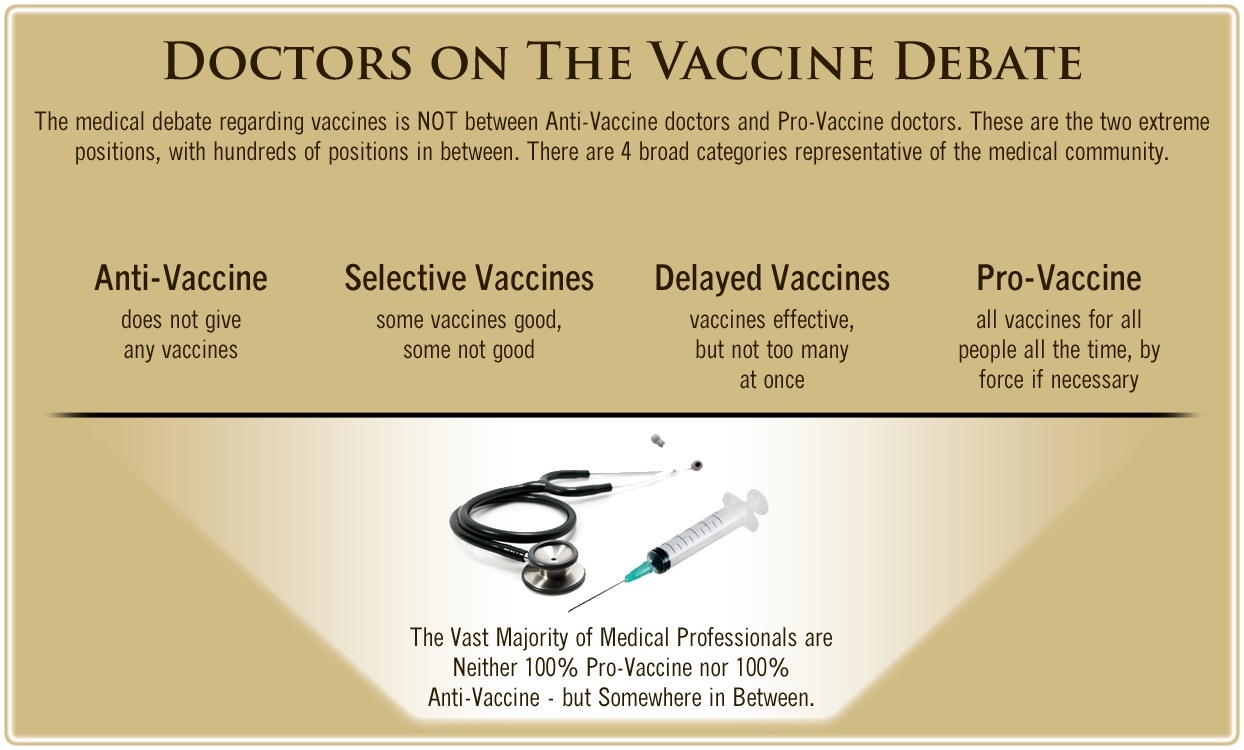
One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.