




ANH-Intl Special Report: COVID-19 – fearmongering born out of uncertainty
By Rob Verkerk PhD, founder, executive and scientific director
Alliance for Natural Health International
Coronavirus 2 or SARS-CoV-2, that causes COVID-19 or just plain old ‘coronavirus’ – call it what you like – has taken the world by storm. Humans in every corner of the globe are coming together to ostensibly minimise human tragedy, suffering and hardship linked to the severe acute respiratory syndrome caused by the new circulating virus. Unwittingly, some of these efforts might actually cause harms they’re intending to prevent. Governments, corporations, transportation companies, schools, the entertainment and sporting sectors – mostly everyone – have accepted that in the absence of a silver, pharmaceutical bullet against this novel viral infective agent, we must accept the cost of the economic impacts caused by our efforts in trying to contain and control transmission.
One positive outcome of the outbreak is the sense of cooperation that has been enabled. Citizens, regardless of geographic borders or background, can contribute, in the words of Tedros Adhanom Ghebreyesus, the Director General of the World Health Organization (WHO),
“to protect themselves, to protect others, whether in the home, the community, the healthcare system, the workplace or the transport system.”
But have health authorities, governments and corporations got enough information and context to be making the decisions they are making, often on our behalf? What are we not being told that we should be told?
Many healthcare professionals working in the natural health or integrative medicine sectors with whom we’ve spoken over the last month or so, like us, feel that context has been sorely missing in the public dialogue on the coronavirus outbreak. As has been comprehensive and relevant advice, especially for older people who are more susceptible, on supporting the immune system (see our separate piece on natural immune support) in the event of infection.
In this special report, released the day after the WHO upgraded the outbreak’s status from epidemic to pandemic, I have attempted to highlight some of the anomalies and problems around the publicly available information, and, just as importantly, identify where key data gaps lie. We hope you’ll find it provides some additional and helpful context to the information that’s being delivered by the mainstream media.
WHO declares pandemic status of COVID-19
Before we kick off proper, if you want to gen up on some basics, albeit from a largely scientific perspective, the following links give you something of a starting point:
- Comparison of COVID-19 and flu by Johns Hopkins
- Key features of COVID-19 outbreak
- Epidemiology and pathogenesis of the COVID-19 outbreak
- Our World in Data – looking at the numbers behind the outbreak
If you already need some light relief, here’s a couple of tidbits of trivia:
- Coronaviruses get their name from the Latin word ‘corona’, which means ‘crown’ or ‘halo’. When you look at them through a 2D transmission electron microscope you see what looks something like a crown comprised of the club-shaped spikes that cover the surface around the virus particles
- Did you know that around 20% of all instances of the common cold are caused by coronaviruses? Unsurprising therefore that most of the symptoms of COVID-19 are something like a common cold
- There’s nothing new about this family of viruses that have co-existed with animals and humans for millennia. This one is called novel because it’s the first time it’s been found in humans. No one can be sure about the origins of the virus, but among the more supported theories is that it jumped from bats to pangolins to humans, where it turned up in the wet market of Wuhan in the Hubei province of China. While the origins remain unclear, there are of course fertile grounds for conspiracy theories. Among them was a view expressed by former Iranian President Mahmoud Ahmadinejad, who sent a letter to the United Nations stating the virus was “a new weapon for establishing and/or maintaining [the] political and economic upper hand in the global arena.”
Microscopic illustration of the spreading 2019 corona virus that was discovered in Wuhan, China. The image is an artisic but scientific interpretation, with all relevant surface details of this particular virus in place, including Spike Glycoproteins, Hemagglutinin-esterase, E- and M-Proteins and Envelope.
WHO said?
Tedros Adhanom Ghebreyesus at the WHO referred to a “sombre moment” as the number of confirmed cases of COVID-19 passed 100,000 in 100 countries over the weekend.
As of yesterday, based on data from Johns Hopkins’ COVID-19 tracker, 87% of cases so far have occurred in just 4 countries (China, Italy, Iran and Korea; see Category 1 countries/areas).
According to the WHO, of the 80,000 reported cases in China, 70% have already fully recovered.
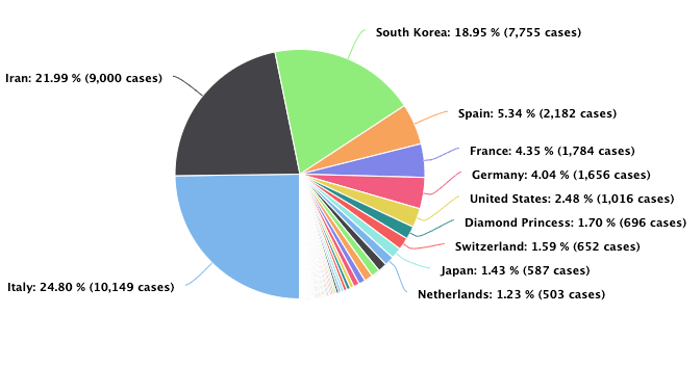
Distribution of cases outside Mainland China as of 11 March 2020. Source: Worldometer
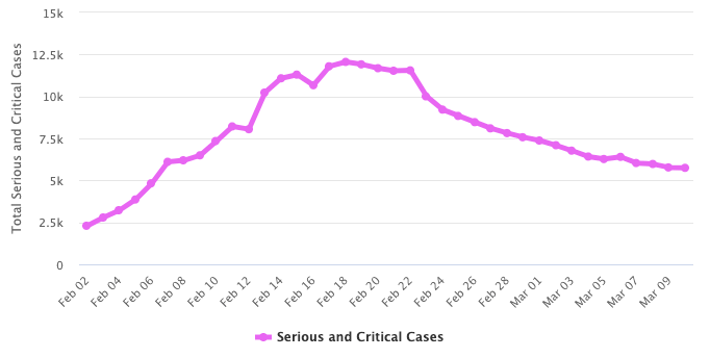
Total serious and critical cases as of 11 March 2020. Source: Worldometer
Context by comparison with other infectious diseases
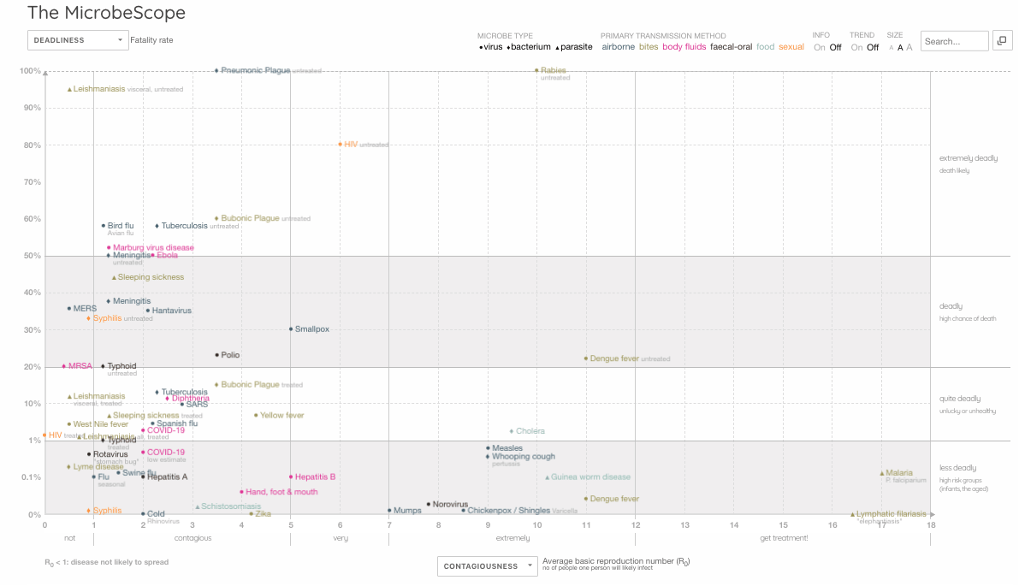
One way of getting context on COVID-19 is to compare the rate of contagiousness (the average basic reproduction number (R0) which is the number of people one person will likely infect) with the case fatality rate (CFR), against other important infectious diseases. This way of looking at the infection makes sense because the COVID-19 outbreak is so recent, while other infectious agents like seasonal flu (caused mostly by influenza A/H1N1 viruses) or ‘swine flu’ (A/H1N1pdm09) have been circulating considerably longer.
One such comparison has been carried out through an interactive graphic called the MicrobeScope (see below) on the Information is Beautiful website. You’ll see data for COVID-19 sitting in the bottom left corner, with moderate contagiousness and relatively low fatality rate (presently around 1-2% of those infected). It’s somewhat higher in Italy (5%), probably because many of those infected have been elderly with comorbidities (heart disease, diabetes, cancer, etc.) so are therefore more susceptible.
You’ll also see, so far, SARS-CoV-2 appears very much less contagious than the mosquito vectored diseases, malaria or dengue fever. It is also much less deadly than tuberculosis, Ebola, meningitis or bird flu, while being slightly more deadly – based on just the first 10 weeks of available data – than seasonal flu.
Link to interactive version of MicrobeScope.
We also need to keep the numbers infected so far in context with those affected by other infectious diseases. Following is a comparison of COVID-19 with 4 other infectious diseases, bearing in mind COVID-19 has reportedly only been circulating for a little over two months:
| Infectious agent | Estimated annual new cases | Estimated related deaths | Source |
| COVID-19 | 113,703* | 4,012* | WHO COVID-2019 situation reports |
| Malaria | 228 million | 405,000 | WHO malaria fact sheet |
| Tuberculosis | ~7 million | 1,491,000 | TBFacts.org |
| Influenza | 3-5 million | 290,000 -650,000 | WHO seasonal influenza fact sheet |
| HIV/AIDS | ~1.7 million | 770,000 | UNAIDS |
*COVID-19 cases only from 31 December 2019 to 10 March 2020.
Other coronaviruses that caused huge public disturbances, albeit in more geographically limited areas, namely China and the Middle East, were the SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome) epidemics of 2002 and 2012, respectively. SARS caused just over 8,000 deaths and had a fatality rate of nearly 10% as against MERS with around 2,500 causes and 834 deaths, amounting to 34% fatality rate. These figures demonstrate just how many more people are being affected by COVID-19, but relatively, how much less harmful it appears to be too. That’s not something the mainstream media often reports in its bid to fearmonger.
Another good way of estimating infection potential is to look at the doubling rate.
Here, for ease, I suggest you look at data collated from official WHO figures by Australian investment guru, Damien Klassen on the website Nucleuswealth. It makes sense if you’re wanting people to invest that you know how a virus like COVID-19 can change market values. Looked at this way, things don’t presently look optimistic in South Korea, Italy and Iran.
Health threat
The trouble is, these bald numbers tell us only a part of the picture. They can also be misleading. When trying to size up the nature of the threat caused by the infectious agents and what priorities you should give to containment and mitigation, you really need solid answers to a lot of questions. These include knowing the age, gender and location of those who’ve died, how many people are infected (including those with and without symptoms), how long it took them to die after infection, did the infection really cause the death or was it just associated with it, what was the lag time between infection and death, what is the reproductive rate of the agent and does this change with time, what was the person’s health status at the time of infection regardless of outcomes, what was the nature and severity of any symptoms….I could go on.
There is data on only some of these parameters. Even less of it is in the public domain.
When you look at the daily stats of escalating infection rates, they tell you nothing about whether lots of these people are recovering from mild symptoms of disease, or were they dying slow, painful deaths in an ICU? Or were they at home or in remote rural areas where they couldn’t gain access to medical care?
What degree of trust can you put in official data being supplied to the WHO? Again, as Damien Klassen suggests, some data can be trusted less than others.
And just how many people out there would be positive if sampled and tested, but they haven’t been tested because they have no symptoms? Take the case of the cruise ship, the Diamond Princess that was docked in Yokohama, Japan. A whopping 52% of the 621 confirmed cases onboard (322) were found to be asymptomatic – according to Japan’s Ministry of Health.
Also, are the laboratory tests being used rock solid, meaning do all positive tests mean the virus is present, and vice versa? Back to the Diamond Princess, why did one women test negative during the two weeks of testing while under quarantine on the boat, only to then be found positive when she returned home in Japan? A similar discovery was subsequently made in the cases of two Australian men.
As you delve into what little is known, and note the mass of information that isn’t, an interesting story emerges, one that is at odds with the more definitive viewpoints underpinning public health policy that are being blasted at us daily across the airwaves.
The likely high (unknown) numbers of unreported cases of infection in part explains why Dr Anthony Fauci, the head of the NIH’s National Institute of Allergy and Infectious Diseases, said in his co-written editorial in the New England Journal of Medicine published on 28 February 2020 that “the case fatality rate may be considerably less than 1%”.
Remember the bird flu pandemic of 2007 caused by the H5N1 virus – or should we say, the human immune reaction to it? At its most virulent, the risk of transmission remained low, relative to many other infectious diseases. The WHO data estimates that the H5N1 avian influenza has killed 53% of those infected between 2003 and 2020, the majority of cases being in just 3 countries, namely Egypt, Indonesia and Vietnam.
However, re-analysis of available data shows that the rate might be closer to 14-33%. This change in fatality rate was linked by the study authors to 3 things: 1) many asymptomatic and mild cases might go unreported, 2) there is common under-reporting by some countries for political reasons, and 3) the virulence, in common with many viral infections, declines over time. All of these concerns apply to COVID-19.
A Chinese study published in The Lancet compared those infected by the novel avian influenza (A/H7N9) which broke out in China in 2013 and the more lethal H5N1 avian influenza virus. It looked at the location and age of infected individuals, among other things. It revealed that the median age of those infected was 62 years for H7N9 and just 26 years for H5N1. In both cases, most of those infected (71-75%) were exposed to poultry.
In Italy, which has seen the highest rate of infection outside of China, the average age of death reported by the country’s national health institute was reported as 81, the majority with underlying health problems and 72% being men.
The WHO continues to uphold the 2% case fatality rate. Prof Neil Ferguson and his team at Imperial College London estimate the case fatality rate (CFR) at half this value, 1% which is close to another assessment by a group of New Zealand experts of a CFR of 1.4% for COVID-19 cases outside China.
But there are problems with all of these estimates. Most of the data we see in peer reviewed papers, being issued by governments and health authorities and in the media are based on confirmed cases provided by national governments to the WHO. This involves cases where there has at least been the matching of viral material taken from nose and throat swabsusing real-time reverse transcription polymerase chain reaction (rRT-PCR).
Being at the early stage of the outbreak, there are limited data on what is happening at a given period in time. For example, if it takes a susceptible person 4 weeks to die following infection, your case-fatality data will be out of step with your infectivity data, being one month behind. The problem is exacerbated further if you have a relatively long incubation time. While varying views on incubation have been put forward, a study just published by Johns Hopkins suggests around a 5-day incubation, which is somewhat shorter than many had previously believed. However, the study also shows that 97.5% of those infected will show symptoms after 11.5 days, while around 1 in 100 will still likely develop symptoms after 14 days of active monitoring or quarantine. Given the infection capacity of COVID-19 and these figures, it’s not hard to see how easily the virus can spread exponentially.

Economic threat
Herein lies the double-edge sword delivered to us by COVID-19. The more humans enact containment and social isolation policies in an effort to slow down the contagion of the virus, the less at risk are the most vulnerable members of our society. But also, the greater is the economic impact. The sheer scale of infection makes it a problem.
SARS had a significantly higher case fatality rate, but much lower rates of infection. It killed only 813 people in total but caused a 2% fall in GDP in China where all but two cases occurred.
The scale of the threat is matched by the size of pledges. The “international community” has asked for US$675 million to help protect states with weaker health systems as part of the WHO Strategic Preparedness and Response Plan.
The Gates Foundation have launched funding to identify COVID-19 treatments in conjunction with Wellcome and Mastercard, with US$125 million being made available.
The UN has released US$15 million from the Central Emergency Response Fund (CERF) to help fund global efforts to contain the COVID-19 virus.
But all this pales into insignificance when you look at the potential impacts on certain industries and economies. One sector that will be hit particularly hard by shutdowns and social isolation policies is the airline industry. The International Air Transport Association (IATA) suggests that as much as US$113 billion might be lost by the airline industry in 2020 alone. While it might be better for the environment, it’s not good for those who benefit from the services provided by the airline industry in linking up the world’s economies.
Back in 2003, SARS cost the world US$40 billion in 6 months. How much more will COVID-19 cost?
Pharma solutions in the pipeline?
No drugs have been proven effective against the virus.
A vaccine is being developed, but Dr. Anthony Fauci (National Institute of Allergy and Infectious Diseases) said it will likely take 12 months before a vaccine is ready for the public, having clashed with US President Donald Trump who said he wanted the vaccine ready in just 2 months.
Gilead Science’s remdesivir is an antiviral drug originally developed against Ebola, which has found use against infections by Marburg and other RNA-stranded viruses. It is currently being trialled in China. It was administered to a US patient on “compassionate grounds” and the patient, whose condition was worsening prior to the drug being given, recovered quickly.
There is a significant risk that mutations by SARS-CoV-2 could lead to resistance to antiviral agents if they were to be used at scale, as occurred with neuraminidase inhibitors like oseltamivir (Tamiflu®) used against seasonal A(H1N1) viral infections.
Useful videos
Prof Neil Ferguson and Prof Christl Donnely (Imperial College London, MRC Centre for Global Infectious Disease Analysis) on current status of COVID-19, containment, and non-pharmaceutical interventions
Dr Seema Yasmin on COVID-19, personal protection and pandemics
Do’s and Don’ts
IMPORTANT NOTICE
The information below is for informational and educational purposes only, and should not be construed as medical advice. If you are experiencing any symptoms of illness, or consider that you might have been exposed to the coronavirus, follow the advice of your health authority [the UK’s NHS advice is fairly detailed and useful wherever you may live]. This will typically mean staying at home and avoiding close contact with other people. Do not go to a GP surgery, pharmacy or hospital and, in the UK, use the NHS 111 coronavirus service to get advice on what to do.
As SARS-CoV-2 is another coronavirus, similar to the type that causes 20% of cases of common cold, the same basic hygiene and sanitation requirements apply and, apart from making sure your immune system is in peak condition to deal with any threats, is your best form of prevention.
The virus is transmitted by droplets or contact.
So, following the CDC non-pharmaceutical advisory makes a lot of sense:
- Wash your hands often with soap and water for 20 seconds, and help young children do the same.
- Cover your nose and mouth with a tissue when you cough or sneeze, then throw the tissue in the trash.
- Avoid touching your eyes, nose, and mouth with unwashed hands.
- Avoid close contact, such as kissing, or sharing cups or eating utensils, with sick people.
- Clean and disinfect frequently touched surfaces, such as toys and doorknobs.
Add to that the NHS guidance, which has only two items in common with the CDC advice (see brackets):
- (wash your hands with soap and water often – do this for at least 20 seconds)
- always wash your hands when you get home or into work
- use hand sanitiser gel if soap and water are not available
- (cover your mouth and nose with a tissue or your sleeve (not your hands) when you cough or sneeze)
- put used tissues in the bin straight away and wash your hands afterwards
- try to avoid close contact with people who are unwell
The don’ts are clearly spelled out by the NHS: “do not touch your eyes, nose or mouth if your hands are not clean.” So there’s a real possibility that if you use a disposable mask, especially a next-to-useless dust mask, you’ll increase, not decrease your risk of infection.
Taking this advice from the CDC and NHS into account, as well as the overall picture of the threat both from infection and from our efforts to mitigate infection, it’s not difficult to consider many reactions to COVID-19 as an over-reaction.
OK – if we’re talking about a very large public meeting for the over-70s in a country or region with known infection by the virus, stop the meeting. Some golf clubs and Bingo halls might be affected, but it won’t bring economies to a standstill. Otherwise, let people get on with their lives, cognisant of the hygiene and sanitation measures. We must also demand more transparency in the reporting.
So keep an eye on the stats, and we’re finding there’s more relevant data delivered daily by Worldometer than there is by the WHO itself.
What the data so far suggest to us is that the vast majority of people (>97%) will be fine, even with infection. Most people will at most have mild symptoms that are not very different from the closely related common cold. Efforts should be made, just as is the case routinely with flu, to in particular protect the most vulnerable groups, especially older people with underlying conditions.
Doing a lot more than all of this right now looks to us like the product of fertile minds and fear-mongering.
Conclusions
COVID-19 has now achieved pandemic status. That label generates fear. Yet the decision is based on geography, not biology. So while some estimates suggest two-thirds of the global population will become infected, for many this might just involve a ‘sniffle and a tickle’ – or be entirely without symptoms.
As stated by the WHO’s Director-General, Tedros Ghebreyesus, “it would be the first pandemic in history that could be controlled.” More importantly, this could be achieved largely without pharmaceuticals or vaccines – just human cooperation around containment and control.
The way things are currently looking, in our view, the biggest cost of the pandemic will not be through suffering and illness. It will be economic. In order to reduce this impact, employers, event managers, transportation companies, health authorities and all those responsible for how those they communicate with behave, need to think things threw very carefully, before knee-jerking.
I was invited to speak at two major conferences next week in London. One has been cancelled (today), the other (at the time of writing) is going ahead. I am impressed with the lead taken by William Reed Business Media Ltd, the publisher of Food Navigator and NutraIngredients, for persevering with the Global CBD Summit and publishing coronavirus safety measures on the website.
I found myself resonating with the commentary in the BMJ offered by Dr Peter Gøtzsche, expelled co-founder of the Cochrane Collaboration and founder of the Institute for Scientific Freedom in Copenhagen. So, let’s finish with Dr Gøtzsche’s words as he explores the notion of us being potential “victims of mass panic”.
He asks:
“Why all the panic? Is it evidence-based healthcare to close schools and universities, cancel flights and meetings, forbid travel, and to isolate people wherever they happen to fall ill? In Denmark, the government recommends cancellation of events with over 1000 participants. When some organisers crept just below 1000, they were attacked by professors in virology and microbiology. But if it is wrong to invite 990 people, it should also be wrong to invite 980, and so forth. Where does this stop? And should big shopping centres be closed, too?”
Read the full article at ANHInternational.org
Comment on this article at HealthImpactNews.com


Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
-
Book – The Vaccine Court, by Wayne Rohde – 240 pages
“The Dark Truth of America’s Vaccine Injury Compensation Program”
FREE Shipping Available!
ORDER HERE!