



Pertussis Microbe Outsmarts the Vaccines As Experts Argue About Why
For the past decade, Americans have been subjected to dire warnings that B. pertussis whooping cough cases are on the rise and it is the fault of parents who don’t vaccinate their children. 1 2 3 That myth actually goes back to the early 1980’s, 4 when parents of DPT vaccine injured children in the U.S. were asking for a safer pertussis vaccine while, at the same time, discovering that whole cell pertussis vaccine in DPT shots did not prevent infection 5 and vaccine immunity lasted for only two to five years. 6 7
The same old excuse – “it’s the parent’s fault” – is being invoked again in the 21stcentury by forced vaccination proponents who want to eliminate vaccine exemptions, 8 9 10 11 just as another generation of parents are discovering that acellular pertussis vaccine in DTaP shots also does not prevent infection 12 13 14 and vaccine immunity is waning, lasting at best for two to five years. 15 16 17
Time to Dispel Myths and Lies About Pertussis and Pertussis Vaccines
What’s old is new again. And it is time to dispel the myths and lies being told about pertussis and pertussis vaccines.
In brief:
- FACT: Both the reactive whole cell DPT vaccine licensed 1949 and the less toxic acellular DTaP vaccine licensed in 1996 do not prevent infection or transmission, and only provide two to five years of temporary immunity at best;
- FACT: Millions of vaccinated children and adults are silently infected with pertussis in the U.S. every year and show few or no symptoms but spread whooping cough to vaccinated and unvaccinated children – without doctors identifying or reporting cases to the government;
- FACT: In response to mass pertussis vaccination campaigns beginning in the 1950s, the B. pertussis microbe evolved to evade both whole cell and acellular pertussis vaccines, creating new strains producing more toxin to suppress immune function and cause more serious disease.
Now, here is the rest of the story in more detail:
High Child Pertussis Vaccination Rates in U.S. for 35 Years
Child pertussis vaccination rates in the U.S. have remained very, very high for the past 35 years. 18 Consistently, more than 94 percent of kindergarten children have had four to five pertussis-containing shots either in whole cell DPT or acellular DTaP vaccines. 19 There is a 94 percent pertussis vaccination rate for children under 35 months old20 and, today, 88 percent of teenagers attending high school have gotten a sixth pertussis booster shot. 21
That’s a lot of pertussis vaccination going on in America for a long time among children of all ages, many of whom are now adults in their 20s, 30s and 40s. So why are public health officials reporting that large numbers of fully vaccinated pre-schoolers in Florida, 22 and fully vaccinated teenagers in California, 23 and fully vaccinated sisters and brothers of newborn infants are spreading pertussis whooping cough – 24 even though most have gotten every pertussis shot recommended by the CDC?
Before we examine why the experts are fighting with each other about the answer to that question, let’s do a quick review of the history of pertussis and pertussis vaccine.
DPT Licensed in 1949 and DTaP in 1996 for U.S. Babies
B. pertussis whooping cough has been around since at least the 16th century, and it can be especially serious for babies who cannot breathe when the sticky mucous produced by the gram negative bacteria clogs their tiny airways. 25 26 The first crude whole cell pertussis vaccine was licensed in 1914, 27 but was not given widely to children until after 1949, when it was combined with diphtheria and tetanus vaccines into the DPT shot 28 and used until 1996, when a less reactive DTaP vaccine was licensed in the U.S. 29
By 2014, public health officials reported that 86 percent of the world’s children had gotten at least three pertussis shots, 30 but estimate there are still about 16 million pertussis cases and 195,000 pertussis-related deaths every year globally. 31
75% Drop in Pertussis Deaths Before DPT Licensed in 1949
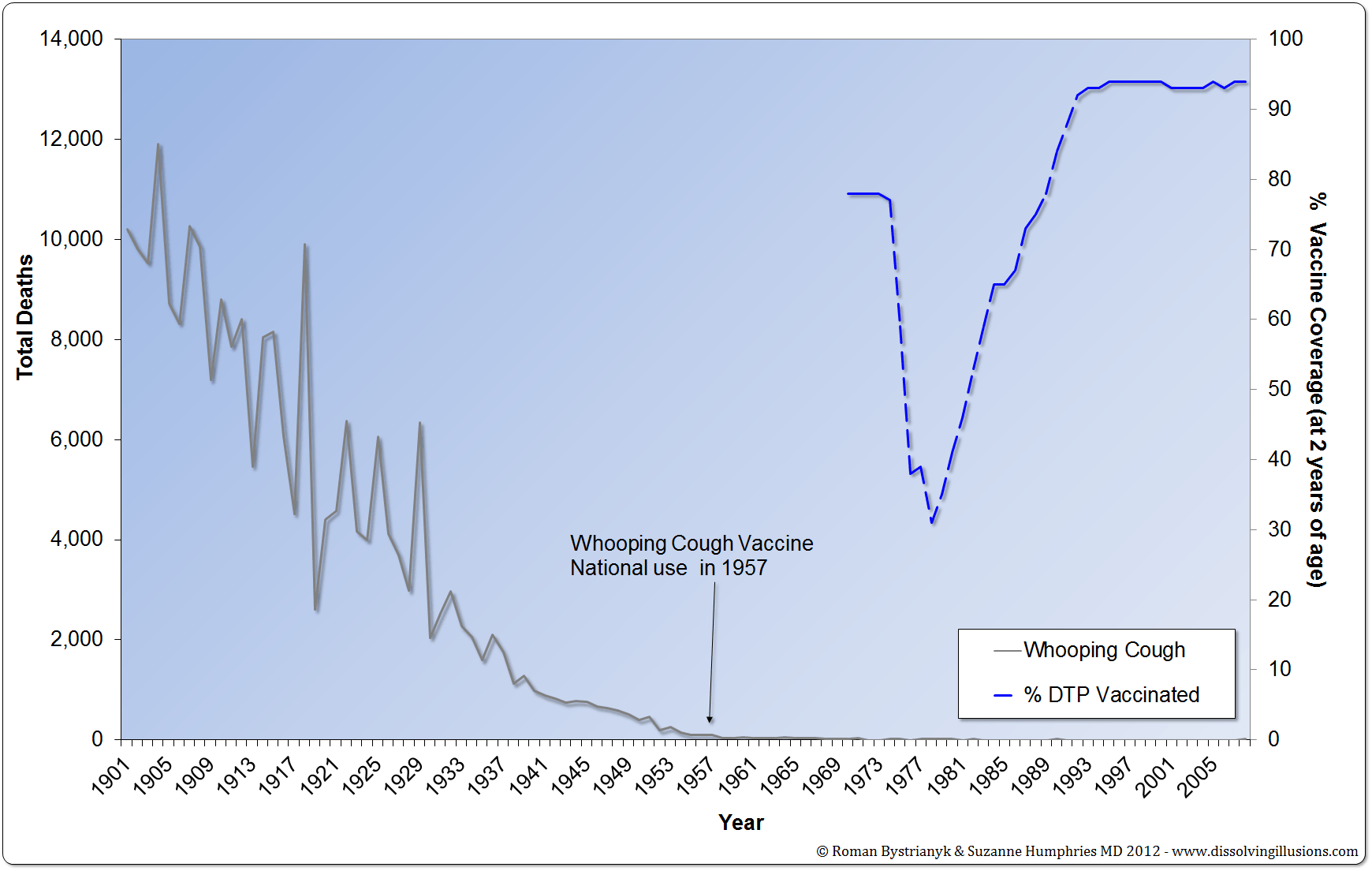
But what about deaths in the U.S. from pertussis whooping cough?
In our country, deaths from pertussis infections dropped by more than 75% between 1922 and 1948, the year before the DPT vaccine was licensed. In 1948, the mortality rate was less than 1 pertussis death per 100,000 persons and would never be higher than that again. 32 33 In 2013, there were about 29,000 reported pertussis cases and 13 pertussis-related deaths in America, with nine of those deaths in infants under age one. 34
However, reported numbers of pertussis cases do not match the total number of actual cases of pertussis that are happening in America. Most pertussis cases, like most vaccine reactions, are not being diagnosed or reported by doctors to the government. 35 Public health officials admit they still don’t have reliable lab tests to measure pertussis immunity and can’t agree about how to diagnose pertussis when infected people, especially vaccinated people, show up in doctor’s offices with mild symptoms.36 37 38
Millions of U.S. Pertussis Cases in Vaccinated Persons Not Identified or Reported
But what public health officials have known for a long time – and do not publicly talk about – is that millions of vaccinated children and adults living in the U.S. get pertussis whooping cough and are never identified. 39 40 41 42 That’s right: there are millions of pertussis infections going on in America among vaccinated people but doctors are not diagnosing or reporting them.
In fact, whether you or your child have been vaccinated or not, you can get a silent asymptomatic pertussis infection and transmit it to someone else without even knowing it. 43 44 45 That child or adult sitting next to you in the bus, classroom, movie theater or doctor’s office, who has a little cough or no cough at all, could be infected with B. pertussis whooping cough, even though he or she has gotten every federally recommended dose of pertussis vaccine.
No Herd Immunity: Vaccines Do Not Block Infection, Carriage or Transmission
When there are a lot of people with silent asymptomatic pertussis infections, it is impossible to know who is a carrier and who is not, which means that reported cases of pertussis are just the tip of a very big iceberg. It also means that articles blaming whooping cough cases on unvaccinated or partially vaccinated children are nothing more than wishful thinking and scapegoating. 46
Bottom Line: Both natural and vaccine acquired immunity is temporary 47and while vaccination may prevent clinical symptoms, it does not block infection, carriage or transmission. If vaccinated people can get silently infected and transmit infection without showing any symptoms – even after getting four to six pertussis shots – then pertussis vaccine acquired “herd immunity” is an illusion and always has been.
So the big question is: Why has more than a half-century of pertussis vaccination failed to produce true herd immunity like public health officials insist it theoretically can if only more and more pertussis shots are given to more people more of the time? 48 49
Extremely Reactive DPT and Less Reactive DTaP both Have Low Efficacy
The answer is simple and the emerging scientific evidence is compelling: the B. pertussis microbe has evolved over the past 65 years to evade whole cell and acellular pertussis vaccines, which drug companies have marketed and medical doctors have aggressively promoted in a crusade to kill a species of bacteria they still know very little about. 50 51 A review of the medical literature reveals that the experts are unhappy with how much they still don’t know about the B. pertussis microbe 52 and are arguing with each other about if, when, how and why pertussis vaccines have consistently failed to do the job of achieving herd immunity to prevent B. pertussis whooping cough from circulating in highly vaccinated populations around the world.53 54 55
The inconvenient set of scientific facts they have to work with are these:
- FACT: The efficacy of whole cell pertussis vaccine in the DPT shot was measured to be between 30 and 85 percent, depending upon the type of DPT and vaccine manufacturer, 56 57 58 59 60 and protection lasted two to five years. 61
- FACT: After a low of about 1,000 cases of pertussis were reported in the U.S in 1976, 62 it was obvious all through the 1980s and 90’s that whole cell pertussis vaccine in DPT shots was not preventing infection or transmission.63 64 65 66 67 Pertussis cases increased in highly vaccinated populations in cycles of three to five years – just like before DPT vaccine was widely used in the 1950s. 68 69 70 71 72
- FACT: The whole cell DPT vaccine used until the late 1990’s in the U.S. was an extremely reactive vaccine. DPT vaccine reactions like fever, pain, and irritability were experienced by between 50 and 85 percent of children and seizures and collapse/shock reactions followed one in 875 DPT shots. 73 74 Brain inflammation was reported following 1 in 110,000 DPT shots with permanent brain damage after 1 in 310,000 DPT shots. 75 76 Finally, in 1996, the marginally effective and extremely reactive whole cell DPT vaccine was replaced with a far less reactive but marginally effective acellular DTaP vaccine. 77 Similar to whole cell pertussis vaccines, acellular pertussis vaccine efficacy in clinical trials was measured to be between 40 and 89 percent, depending upon the DTaP vaccine manufacturer. 78 79 80
- FACT: Acellular pertussis vaccines do not prevent infection, 81 82 just like whole cell pertussis vaccines do not prevent infection. In the 21st century, pertussis outbreaks and cyclical increases have continued,83 84 85 – even after a pertussis booster shot was added to the schedule for all adolescents and adults in 2006. 86 87 By 2010, the Tdap pertussis booster shot was found to be only about 66 percent effective in providing temporary immunity for teenagers and adults. 88
Pertussis Microbe Evolved to Evade Both DPT and DTaP Vaccines
Eighteen years ago, in 1998, molecular biologists and other basic science researchers began warning that the B. pertussis microbe started to evolve to evade whole cell pertussis vaccine after DPT shots were given on a mass basis to children in the 1950’s.89 90 91 92 For the past two decades, these bench scientists have been publishing hard evidence that over the past 65 years, B. pertussis bacteria have efficiently adapted to both whole cell and acellular pertussis vaccines. 93 94 95
New Pertussis Strains with More Toxin Causing More Serious Disease
In a fight to survive, the B. pertussis microbe has created new strains that produce more pertussis toxin to suppress the human immune system and cause more serious disease. Today, the pertussis strains included in the vaccine no longer match the pertussis strains causing whooping cough disease.96 97 98 99 100
Bottom line: There is compelling scientific evidence that B. pertussis bacteria have evolved to survive vaccine pressure. Now, there are more virulent pertussis strains that are more efficiently transmitted by vaccinated children and adults with waning immunity.
As one research scientist commented in 2009, “An important question is whether other childhood vaccines also select for pathogens that are more efficiently transmitted by primed hosts, resulting in increased virulence.” 101
War on B. Pertussis Bacteria & Vaccine Policies Not Driven By Hard Science
The crusade by public health officials to kill the B. pertussis microbe by adding more and more doses of ineffective vaccines to the child and adult schedule – now even invading the once sacred place of the womb and insisting all pregnant women be vaccinated 102 103 – is a cautionary tale. As we witness a bacterial species efficiently adapting in an effort to survive a war that has been declared on it, what has become painfully clear is that the history of mass vaccination has not been driven by hard science transparently shared with the people. 104 105 It has been driven by the politics of a public health profession working a lucrative government-industry public private partnership to protect failed vaccine policies, while ignoring the hard science. 106 107
We, the people, are not going to pretend the science doesn’t exist. It is up to each one of us to inform public health officials and legislators that it is their responsibility to show us the science and give us a choice when it comes to vaccines, especially when no vaccine manufacturer, no public health official and no doctor is liable in a civil court of law when vaccine reactions and failures lead to injury and death. 108
Learn more on NVIC.org. Sign up for the free NVIC Advocacy Portal and become active in your state to protect vaccine exemptions from being eliminated by the Pharma, Medical Trade and Public Health industries.
It’s your health. Your family. Your choice.

Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?

One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.
Sources and References
1 MSNBC. Growing outbreaks of whooping cough raise health fears . July 28, 2010.
2 Brown M. Pertussis Outbreaks Hit West, Midwest – Again. Parents Refusal to Vaccinate Singled Out as Contributing Factor . American Academy of Family Physicians (AAFP). May 30, 2012.
3 Kerns J. Researchers: Vaccination Exemptions Linked to Increase in Whooping Cough Cases. MyNorthwest.comJune 4, 2013.
4 Kotulak R. Vaccination Urged for Whooping Cough . Chicago Tribune. Nov. 17, 1985.
5 Fine PEM, Clarkson JA. The Recurrence of Whooping Cough: Possible Implications for Assessment of Vaccine Efficacy . The Lancet 1982; 1(8273): 666-669.
6 Trollfors B. Bordetella pertussis whole cell vaccines – efficacy and toxicity . Acta paediatrica Scandinavia 1984; 73(4): 417-425.
7 Transcript (partial) of May 12, 1986 ACIP Meeting discussion of DPT risks and failures. Pgs. 34-37. NVIC.org.
8 Stadlin S, Bednarczyk RA, Omer SB. Medical Exemptions to School Immunization Requirements in the United States – Association of State Policies with Medical Exemption Rates (2004-2011). J Infect Dis Aug. 29, 2012.
9 Omer SB. How to Handle the Vaccine Skeptics. The New York Times Feb. 6, 2015.
10 Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. Association Between Vaccine Refusal and Vaccine-Preventable Disease in the United States: A Review of Measles and Pertussis. JAMA 2016; 315(11): 1149-1158.
11 Rappaport L. Vaccine refusal tied to increased risk of measles and pertussis. Reuters Mar. 15, 2016.
12 Lavine J, Bjornstad O, de Blasio BF, Storsaeter J. Short-lived immunity against pertussis, age-specific routes of transmission, and the utility of a teenage booster vaccine . Vaccine 2012; 30(3): 544-551.
13 Cherry JD. Why Do Pertussis Vaccines Fail? Pediatrics 2012; 129(5).
14 Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc Natl Acad Sci USA. 2014; 111(2): 787–792
15 Misegades LK, Winter K, Harriman K et al. Association of Childhood Pertussis With Receipt of 5 Doses of Pertussis Vaccine by Time Since Last Vaccine Dose, California, 2010 . JAMA 2012; 308(20): 2126-2132.
16 Matthias J, Pritchard S, Martin SW et al. Sustained Transmission of Pertussis in Vaccinated, 1–5-Year-Old Children in a Preschool, Florida, USA . Emerging Infectious Diseases Jan. 15, 2016.
17 Klein NP, Bartless S, Fireman B, Baxter R.Waning Tdap Effectiveness in Adolescents. Pediatrics Feb. 3, 2016.
18 Hinman A, Orenstein WA, Schuchat A.Vaccine Preventable Diseases, Immunization and MMWR 1961-2011.MMWR Oct. 7, 2011; 60(04): 49-57.
19 CDC. Vaccination Coverage Among Children in Kindergarten – United States, 2014-15 School Year . Aug. 28, 2015: 64(33): 897-904.
20 CDC. National, State and Selected Local Area Vaccination Coverage Among Children Aged 19-36 Months – United States, 2014 . Aug. 28, 2015: 64(33): 889-896.
21 CDC. National, Regional, State and Selected Local Area Vaccine Coverage Among Adolescents Aged 13 to 17 Years – United States, 2014 . MMWR 2015; 64(29): 784-792.
22 Matthias J, Pritchard S, Martin SW et al. Sustained Transmission of Pertussis in Vaccinated, 1–5-Year-Old Children in a Preschool, Florida, USA . Emerging Infectious Diseases Jan. 15, 2016.
23 Klein NP, Bartless S, Fireman B, Baxter R.Waning Tdap Effectiveness in Adolescents. Pediatrics Feb. 3, 2016.
24 Skoff TH, Kenyon C, Cocoros N et al. Sources of Infant Pertussis Infection in the United States. Pediatrics 2015; 136(4): 635-641.
25 Bart MJ, Harris SR, Advani A et al. Global Population Structure and Evolution of Bordetella pertussis and Their Relationship with Vaccination . MBio 2014; 5(2).
26 Kallonen T, He Q. Bordetella pertussis strain variation and evolution post vaccination. Expert Rev Vaccines 2009; 8(7): 863-875.
27 Institute of Medicine. Pertussis and Rubella Vaccines: A Brief Chronology (Appendix B, pp. 320) In: Adverse Effects of Pertussis and Rubella Vaccines. The National Academies Press 1991.
28 NIH. Historical Record of Vaccine Product Licensing Holders in the United States. (Table H-1). In: The Children’s Vaccine Initiative: Achieving the Vision. The National Academy of Sciences 1993.
29 CDC. Pertussis vaccination: use of acellular pertussis vaccines among infants and young children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Mar. 28, 1997;46(RR-7):1–25
30 World Health Organization. Immunization Coverage (Global). WHO September 2015.
31 CDC. Pertussis in Other Countries. Sept. 8, 2015.
32 National Center for Health Statistics. U.S. Vital Statistics Mortality Data 1940-1949. Table 2 – Death Rates for Selected Causes, Whooping Cough (All Races, Both Sexes) 1948 . Pg. 38.
33 Grove RD, Hetzel AM. Vital Statistics Rates in the United States 1940-1960. General Mortality (1921-1929), Section C, Table 65: Whooping Cough . Pg. 577. U.S. Public Health Service National Center for Health Statistics1968.
34 CDC. 2013 Final Pertussis Surveillance Report. Aug. 15, 2014.
35 ` Bamberger ES, Srugo I. What is new in pertussis? Eur J Pediatr 2008; 167: 133-139.
36 Cherry JD. Why Do Pertussis Vaccines Fail? Pediatrics 2012; 129(5).
37 Zouari A, Smaoui H, Kechrid A. The diagnosis of pertussis: which method to choose? Crit Rev Microbiol 2012; 38(2): 111-121.
38 Van der Zee A, Schellekens JF, Mooi FR. Laboratory Diagnosis of Pertussis. Clin Microbiol Rev 2015; 28(4): 1005-10026.
39 Sutter RW, Cochi SL. Pertussis Hospitalizations and Mortality in the United States, 1985-1988: Evaluation of the Completeness of National Reporting . JAMA 1992; 267(3): 386-391.
40 Deville JG, Cherry JD, Christenson PD et al.Frequency of Unrecognized Bordetella pertussis Infections in Adults.Clin Infect Dis 1995; 12: 639-642
41 Cherry JD. The Epidemiology of Pertussis: A Comparison of the Epidemiology of the Disease Pertussis With the Epidemiology of Bordetella pertussis Infection . Pediatrics 2005; 115(5).
42 Ward JI, Cherry JD, Chang S et al.Efficacy of an Acellular Pertussis Vaccine among Adolescents and Adults. N Eng J Med 2005; 353(15): 1555-1563.
43 Long SS, Lischner HW et al.Serologic evidence of subclinical pertussis in immunized children. Pediatr Infect Dis1990; 9(10): 700-705.
44 He Q, Viljanen MK, Nikkari S et al. Outcomes of Bordetella pertussis Infection in Different Age Groups in an Immunized Population . J Infect Dis 1994; 170: 873-877.
45 Zhang Q, Yin Z, Shao LH et al. Prevalence of asymptomatic Bordetella pertussis and Bordetella parapertussis infections among school children in China as determined by pooled real-time PCR: a cross-sectional study . Scand J Infect Dis 2014; 46(4): 280-287.
46 Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. Association Between Vaccine Refusal and Vaccine-Preventable Disease in the United States: A Review of Measles and Pertussis. JAMA 2016; 315(11): 1149-1158.
47 Wendelboe AM, Van Rie A et al.Duration of immunity against pertussis after natural infection or vaccination.Pediatr Infect Dis J 2005; 24(Suppl 5): S58-S61.
48 Wei SC, Tetti K, Cushing K et al. Effectiveness of Adolescent and Adult Tetanus Reduced-Dose Diphtheria and Acellular Pertussis Vaccine against Pertussis . Clin Infect Dis 2010; 51(3): 315-321.
49 Gabutti G, Azzari C, Bonanni P et al.Pertussis: Current perspectives on epidemiology and prevention. Human Vaccines & Immunotherapeutics 2015; 11(1): 108-117.
50 Coote JG. Environmental sensing mechanisms in Bordetella. Adv Microb Physiol 2001; 44: 141-181.
51 Melvin JA, Scheller EV et al. Bordetella pertussis pathogenesis: current and future challenges . Nature Reviews Microbiology 2014; 12: 274-288.
52 Hewlett EK, Burns DL Cotter PA et al.Pertussis Pathogenesis – What We Know and What We Don’t Know. J Infect Dis 2014; 209: 982-985.
53 Robbins JB, Schneerson R, Kubler-Kielb J et al. Toward a new vaccine for pertussis. PNAS 2014; 111(9): 3213-3216.
54 Riolo MA, Rohani.Combating pertussis resurgence: One booster vaccination schedule does not fit all. Proc Nat Acad Sci 2015; 112(5): E472-477.
55 De Celles MD, Magpantay FMG et al.The pertussis enigma: reconciling epidemiology, immunology and evolution. Proc R Soc B 2016; 283.
56 Preston NW, Stanbridge TN. Efficacy of Pertussis Vaccines: A Brighter Horizon. Brit Med J 1972; 3:448-451.
57 Broome CV, Preblud SR, Bruner B et al. Epidemiology of pertussis, Atlanta, 1977. J Pediatr 1981; 98(3): 362-267.
58 Fine PE, Clarkson JA. Reflections on the efficacy of pertussis vaccines. Rev Infect Dis 1987; 9(5): 866-883.
59 Greco D, Salmaso S, Mastrantonio P et al. A Controlled Trial of Two Acellular Vaccines and One Whole-Cell Vaccine Against Pertussis . N Engl J Med 1996; 334(6): 341-348.
60 Schmitt HJ, Schuind A, Knuf M et al. Acellullar Pertussis Vaccines: The Rationale for an Efficacy Trial in Germany . J Infect Dis 1996; 174(Suppl 3): S287-S290.
61 Trollfors B. Bordetella pertussis whole cell vaccines – efficacy and toxicity . Acta paediatrica Scandinavia 1984; 73(4): 417-425.
62 CDC. Pertussis (Whooping Cough) Cases by Year (1922-2014). Sept. 8, 2015.
63 Fine PEM, Clarkson JA. The Recurrence of Whooping Cough: Possible Implications for Assessment of Vaccine Efficacy . The Lancet 1982; 1(8273): 666-669.
64 Marchant CD, Loughlin AM, Lett SM et al. Pertussis in Massachusetts, 1981-1991: incidence, serologic diagnosis, and vaccine effectiveness . J Infect Dis 1994; 169(6): 1297-1305.
65 Tanaka M, Vitek CR, Pascual B et al.Trends in Pertussis Among Infants in the United States, 1980-1999. JAMA2003; 290)22): 2968-2975.
66 Nelson JD. The changing epidemiology of pertussis in young infants. The role of adults as reservoirs of infection . Am J Dis Child 1978 132(4): 371-373.
67 Yih WK, Lett SM, desVignes FN et al. The increasing incidence of pertussis in Massachusetts adolescents and adults 1989-1998 . J Infect Dis 2000; 182(5): 1409-1416.
68 Christie CDC, Marx ML, Colin D et al. The 1993 Epidemic of Pertussis in Cincinnati. N Engl J Med 1994; 331: 16-21.
69 DeSerres G, Boulianne N et al. Pertussis in Quebec: ongoing epidemic since the late 1980’s . Can Commun Dis Rep 1995; 21(5): 45-48.
70 CDC. Pertussis Outbreak – Vermont, 1996. MMWR Sept. 5, 1997; 46(35): 822-826.
71 Jenkinson D. Duration of effectiveness of pertussis vaccine: evidence form a 10 year community study . Brit Med J1988; 296: 612-614.
72 Bouchez B, Guiso N. Bordetella pertussis, B. parapertussis, vaccines and cycles of whooping cough. FEMS Pathogens and Disease Aug. 4, 2015 (online).
73 Barkin RM, Pichichero ME. Diphtheria-Pertussis-Tetanus Vaccine: Reactogenicity of Commercial Products. Pediatrics 1979; 63(2).
74 Cody CL, Baraff LJ, Cherry JD et al. Nature and Rates of Adverse Reactions Associated with DTP and DT Immunizations in Infants and Children . Pediatrics 1981; 68(5).
75 Miller DL, Ross EM, Alderslade R et al.Pertussis immunization and serious acute neurological illness in children.Brit Med J 1981; 282: 1595-1599.
76 Institute of Medicine. DPT Vaccine and Chronic Nervous System Dysfunction: A New Analysis. Washington, D.C. The National Academies Press 1994.
77 CDC. Pertussis vaccination: use of acellular pertussis vaccines among infants and young children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Mar. 28, 1997;46(RR-7):1–25
78 Gustafsson L, Hallander HO, Olin P et al. A Controlled Trial of a Two-Component Acellular, A Five-Component Acellular, and a Whole Cell Pertussis Vaccine . New Engl J Med1996; 334(6): 349-355.
79 Greco D, Salmaso S, Mastrantonio P et al. A Controlled Trial of Two Acellular Vaccines and One Whole-Cell Vaccine Against Pertussis . N Engl J Med 1996; 334(6): 341-348.
80 Zhang L, Prietsch SOM et al. Acellular vaccines for preventing whooping cough in children (Review). The Cochrane Library 2014 , Issue 9.
81 Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc Natl Acad Sci USA. 2014; 111(2): 787–792.
82 Lavine J, Bjernstad O, de Blasio BF, Storsaeter J. Short-lived immunity against pertussis, age-specific routes of transmission, and the utility of a teenage booster vaccine . Vaccine 2012; 30(3): 544-551.
83 DeGouw D, Diavatopoulos DA, Bootsma HJ et al. Pertussis: a matter of immune modulation. FEMS Microbiol Rev2011; 35(2011): 441-474.
84 Libster R, Edwards KM. Re-emergence of Pertussis: What Are the Solutions? Expert Rev Vaccines 2012; 11(11): 1331-1346.
85 Bouchez B, Guiso N.Bordetella pertussis, B. parapertussis, vaccines and cycles of whooping cough. FEMS Pathogens and Disease Aug. 4, 2015 (online
86 CDC. Preventing Tetanus, Diphtheria, and Pertussis Among Adolescents: Use of Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccines. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR May 24, 2006;55(RR-3):1–34.
87 CDC. Preventing Tetanus, Diphtheria, and Pertussis Among Adults: Use of Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccines. Recommendations of the Advisory Committee on Immunization Practices (ACIP) and Recommendation of ACIP supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC for Use of Tdap Among Health-Care Personnel. MMWR Dec. 15, 2006; 55(RR-17): 1-37.
88 Wei SC, Tetti K, Cushing K et al. Effectiveness of Adolescent and Adult Tetanus Reduced-Dose Diphtheria and Acellular Pertussis Vaccine against Pertussis . Clin Infect Dis 2010; 51(3): 315-321.
89 Mooi FR, van Oirschot H, Heuvelman K et al. Polymorphism in the Bordetella pertussis Virulance Factors P. 69/Pertactin and Pertussis Toxin in The Netherlands: Temporal Trends and Evidence for Vaccine-Driven Evolution . Infection and Immunity 1998; 66(2): 670-675.
90 Simondon F., Guiso N.Genetic evolution under vaccine pressure: the Bordetella pertussis model. Bull Soc Pathol Exot 2000; 93(3): 202-205.
91 De Melker HE, Schellekens JFP, Neppelenbroek SE et al. Reemergence of Pertussis in the Highly Vaccinated Population of the Netherlands: Observations on Surveillance Data. Emerg Infect Dis 2000; 6(4): 348-357.
92 Mooi FR, vanLoo IHM, King AJ . Adaptation of Bordetella pertussis to vaccination: A Cause for Its Reemergence? Emerg Infect Dis 2001; 7(3): 526-528.
93 Weber C, Boursaux-Eude C, Coralie G et al. Polymorphism of Bordetella pertussis Isolates Circulating for the Last 10 Years in France, Where a Single Effective Whole-Cell Vaccine Has Been Used for More than 30 Years . J Clin Microbiol 2001; 39(12): 4296-4403.
94 Bart MJ, van Gent M, van der Heide HGJ et al. Comparative genomics of prevaccination and modern Bordetella pertussis strains . BMC Genomics 2010; 11: 627.
95 Xu Y, Liu B et al. Whole-genome sequencing reveals the effect of vaccination on the evolution of Bordetella pertussis . Sci Rep 2015; 5: 12888.
96 Mooi FR, van Loo IHM, van Gent M et al. Bordetella pertussis Strains with Increased Toxin Production Associated with Pertussis Resurgence . Emerg Infect Dis 2009; 15(8): 1206-1213.
97 Kallonen T, He Q. Bordetella pertussis strain variation and evolution post vaccination. Expert Rev Vaccines 2009; 8(7): 863-875.
98 Mooi FR. Bordetella pertussis and vaccination: the persistence of a genetically monomorphic pathogen . Infect Genet Evol 2010; 10(1): 36-49.
99 Guiso N, Hegerle N. Other Bordetellas, lessons for and from pertussis vaccines. Expert Rev Vaccines 2014; 13(9): 1125-1133.
100 Bouchez V, Hegerle N, Strati F et al.New Data on Vaccine Antigen Deficient Bordetella pertussis Isolates.Vaccines (Basel) 2015; 3(3): 751-770.
101 Mooi FR, van Loo IHM, van Gent M et al. Bordetella pertussis Strains with Increased Toxin Production Associated with Pertussis Resurgence . Emerg Infect Dis 2009; 15(8): 1206-1213.
102 CDC. Updated Recommendations for Use of Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine (Tdap) in Pregnant Women and Persons Who Have or Anticipate Having Close Contact with an Infant Aged <12 Months — Advisory Committee on Immunization Practices (ACIP), 2011 . MMWR Oct. 21, 2011; 60(41): 1424-1426.
103 Healy CM, Rench MA, Wootton SH, Castagnini LA.Evaluation of the impact of a pertussis cocooning program on infant pertussis infection. Pediatr Infect Dis J 2015; 34(1): 22-26.
104 NVIC. National Vaccine Information Center Supports Three of Five Recommendations of New IOM Report on U.S. Childhood Immunization Schedule Safety and Calls for Transparency. Businesswire Jan. 16, 2013.
105 Collins F. Resurgence of Measles, Pertussis Fueled by Vaccine Refusals . NIH Mar. 22, 2016.
106 Fisher BL. The Vaccine Culture War in America: Are You Ready? NVIC Newsletter Mar. 8, 2015.
107 NVIC. National Vaccine Information Center Says Proposed 21st Century Cures Act Will Endanger the Public Health by Lowering FDA Licensing Standards . Businesswire July 22, 2015.
108 Fisher BL. Vaccine Injury Compensation: Government’s Broken Social Contract with Parents. Nov. 2, 2015. NVIC Newsletter Nov. 2, 2016.
Read the full article at NationalVaccineInformationCenter.org
Leave a Reply