



High-Risk HPV Type Replacement Follows HPV Vaccination
by James Lyons-Weiler, PhD
World Mercury Project
The number of studies that show that partial immunization via available HPV (human papillomavirus) vaccines is not only insufficient at reducing overall HPV infection rates; the vaccines actually cause rarer, more lethal types of HPV to sweep in and the net effect could be devastating increases in HPV-related cancers.
Here I review the biomedical research studies that show that type replacement is real, and that vaccination against the more common types may be, sadly and ironically, expected to cause INCREASES in HPV-related cancer.
The first study is Center for Disease Control’s (CDC) own study, in which they show no net change in HPV infection rate (considering all types) after HPV vaccines were introduced into medical practice:
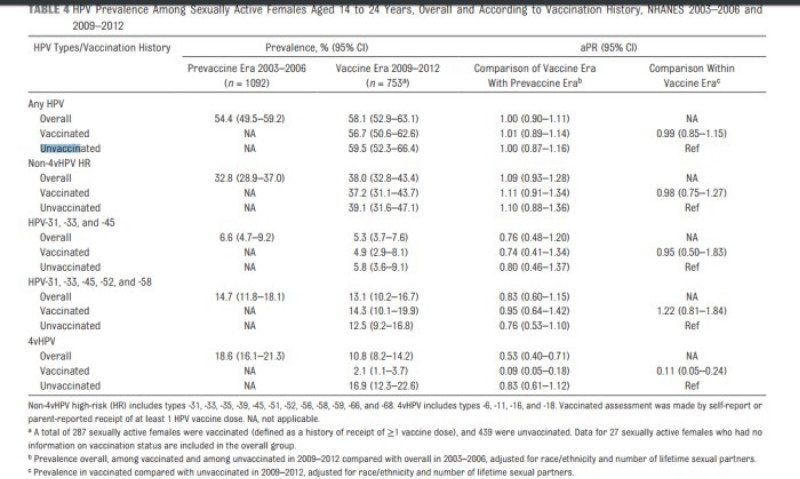
Markowitz LE et al., 2016 Prevalence of HPV After Introduction of the Vaccination Program in the United States. Pediatrics. 2016 Feb 22. pii: peds.2015-1968.
That study concluded that type replacement did not occur because their univariate analysis of individual types showed no individual type with a significant increase. However, because the vaccines do clear the vaccine-targeted types, the lack of change in overall infection rate shows that type replacement must be occurring.
The second study is by Fisher et al. (2016), which specifically found that high-risk HPV types replaced the vaccine-targeted types. They wrote:
“the percentage of non-vaccine HR-HPV types was higher than expected, considering that eight HPV types formerly classified as ‘low-risk’ or ‘probably high-risk’ are in fact HR-HPV types.”
Fischer et al 2016: Shift in prevalence of HPV types in cervical cytology specimens in the era of HPV vaccination. Oncol Lett. 12(1):601-610.
A third study is that by Guo et al., (2015) that also clearly found evidence of type replacement occurring as a result of HPV vaccination:
“The prevalence of high-risk nonvaccine types was higher among vaccinated women than unvaccinated women (52.1% vs 40.4%, prevalence ratio 1.29, 95% CI 1.06–1.57), but this difference was attenuated after adjusting for sexual behavior variables (adjusted prevalence ratio 1.19, 95% CI 0.99–1.43). HPV vaccination was effective against all 4 vaccine types in young women vaccinated after age 12. However, vaccinated women had a higher prevalence of high-risk nonvaccine types, suggesting that they may benefit from newer vaccines covering additional types.”
Guo et al., 2015. Comparison of HPV prevalence between HPV-vaccinated and non-vaccinated young adult women (20-26 years) American Association for Cancer Research Meeting, Apr 18-22; Philadelphia, PA. Philadelphia (PA): AACR; 2015. Abstract nr 844
A fourth study is that by Mollers et al., who wrote
“…our findings do suggest that clustering differs among HPV types and varies across risk groups.”
and
“The ecological niche could also be taken through type replacement, which refers to the possibility that elimination of HPV16 and HPV18 could lead to an increased transmission of nonvaccine types. For this to occur, antagonistic interactions are required between vaccine types and those not included in the vaccine (8, 9). Type replacement has been observed following vaccination against other pathogens (e.g., Streptococcus pneumoniae) (10) and is plausible whenever genotypically diverse pathogen strains compete for the same hosts.”
Mollers M et al., 2014. Population- and type-specific clustering of multiple HPV types across diverse risk populations in the Netherlands. Am J Epidemiol. 179(10):1236-46. doi: 10.1093/aje/kwu038.
A study of Italian women also considered type replacement and wrote that “an accurate post-vaccine surveillance is necessary to early detect a possible genotype replacement.”
Giambi C et al., 2013. A cross-sectional study to estimate high-risk human papillomavirus prevalence and type distribution in Italian women aged 18-26 years. BMC Infect Dis. 13:74. doi: 10.1186/1471-2334-13-74.
…studies now from the US, Germany, Italy and the Netherlands all support the same conclusions: there is evidence for grave concern over the adequacy of HPV vaccines: while the vaccine-targeted types are cleared, the hundred or so that can replace them across the sexually active population includes pathogenic types that may be more lethal than those targeted by the vaccines.
There are other studies that show type replacement. While some studies may show no type replacement, negative results do not take precedence over positive results.
At best, one could say that the science is unsettled. However, CDC’s own study showed no net change in HPV infection rate, and studies now from the US, Germany, Italy and the Netherlands all support the same conclusions: there is evidence for grave concern over the adequacy of HPV vaccines: while the vaccine-targeted types are cleared, the hundred or so that can replace them across the sexually active population includes pathogenic types that may be more lethal than those targeted by the vaccines.
The statistics on the types that are said to be known to cause the most cancers are potentially misleading, because there is an inverse relationship between the ability of the pathogen to cause disease (morbidity) and death (mortality). If you count numbers of cases, yes, HPV-16 appears to be high-risk. But the low-frequency types may be even HIGHER risk – which would explain why they are low-frequency.
The study from Germany (Fisher et al., 2016) is definitive, and we have our answer: HPV type replacement is real, and is caused by partial vaccination against an oncogenic virus group.
About the author
Dr. James Lyons-Weiler, PhD is the author of several books, including “Ebola: An Evolving Story,” “Cures vs. Profits: Successes in Translational Research,” and “The Environmental and Genetic Causes of Autism.” He is the CEO and Director of IPAK, The Institute for Pure and Applied Knowledge, a not-for-profit pure public charity research institute focused on the reduction of human pain and suffering. You can support IPAK and its various projects, studies and initiatives at ipaknowledge.org. You can read more of Dr. Lyons-Weiler’s analyses at jameslyonsweiler.com and find his peer-reviewed publications at PubMed.
Read the Full Article at WorldMercuryProject.org.

Young women whose lives were destroyed by the HPV vaccine.
California Nurse Gives Gardasil Vaccine to Own Daughter who Develops Leukemia and Dies
Infant Accidentally Vaccinated with Gardasil – Mother Blamed for Vaccine Injuries and Baby Medically Kidnapped
Iowa Girl Faces Death: Life Destroyed by Gardasil Vaccine
Gardasil Vaccine Given without Consent and Ruins Life of 14 Year Old Girl
After 3 Years of Suffering 19 Year Old Girl Dies from Gardasil Vaccine Injuries
Gardasil: The Decision We Will Always Regret
The Gardasil Vaccine After-Life: My Daughter is a Shadow of Her Former Self
Gardasil: An Experience no Child Should Have to Go Through
I Want my Daughter’s Life Back the Way it was Before Gardasil
Gardasil Vaccine: Destroyed and Abandoned
15-Year-Old Vaccinated by Force with Gardasil now Suffers from Paralysis and Pain
Recovering from my Gardasil Vaccine Nightmare
Gardasil: We Thought It Was The Right Choice
“HPV Vaccine Has Done This to My Child”
13 Year Old World Championship Karate Student Forced to Quit After Gardasil Vaccine
If I Could Turn Back Time, Korey Would not Have Received any Gardasil Shots
What Doctors Don’t Tell You: Our Gardasil Horror Story
Family Fights U.S. Government over Compensation for Gardasil Vaccine Injuries
Gardasil: When Will our Nightmare End?
HPV Vaccine Injuries: “I Cannot Begin to Describe What it is Like to Watch your Daughter Live in Such Agony”
Gardasil: Don’t Let Your Child Become “One Less”
The Gardasil Vaccine Changed Our Definition of “Normal”
Gardasil: I Should Have Researched First
“They’ve Been Robbed of Their Womanhood” – Local Milwaukee Media Covers Gardasil Vaccine Injuries
Gardasil: The Day Our Daughter’s Life Changed
Gardasil: The Decision I will Always Regret
Gardasil Vaccine: One More Girl Dead
Gardasil: A Parent’s Worst Nightmare
After Gardasil: I Simply Want my Healthy Daughter Back
Gardasil: My Family Suffers with Me
Gardasil Changed my Health, my Life, and Family’s Lives Forever
Gardasil: Ashlie’s Near-Death Experience
Gardasil: My Daughter’s Worst Nightmare
My Personal Battle After the Gardasil Vaccine
Gardasil: The Worst Thing That Ever Happened to Me
A Ruined Life from Gardasil
HPV Vaccines: My Journey Through Gardasil Injuries
The Dark Side of Gardasil – A Nightmare that Became Real
Toddler Wrongly Injected with Gardasil Vaccine Develops Rare Form of Leukaemia
More information about Gardasil

Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?

One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.

One Comment