




by Brian Shilhavy
Editor, Health Impact News
A major study has just been published in the Journal of Toxicology and Environmental Health looking at declining fertility rates among eight million U.S. women aged 25 to 29 during a 7-year period.
The title of study, published by Gayle DeLong, Ph.D., from the Department of Economics and Finance, Baruch College/City University of New York, is “A lowered probability of pregnancy in females in the USA aged 25–29 who received a human papillomavirus vaccine injection.”
From the abstract:
This study analyzed information gathered in National Health and Nutrition Examination Survey, which represented 8 million 25-to-29-year-old women residing in the United States between 2007 and 2014.
Approximately 60% of women who did not receive the HPV vaccine had been pregnant at least once, whereas only 35% of women who were exposed to the vaccine had conceived.
Using logistic regression to analyze the data, the probability of having been pregnant was estimated for females who received an HPV vaccine compared with females who did not receive the shot.
Results suggest that females who received the HPV shot were less likely to have ever been pregnant than women in the same age group who did not receive the shot. If 100% of females in this study had received the HPV vaccine, data suggest the number of women having ever conceived would have fallen by 2 million.
Corporate Media Censorship: Why Isn’t This Study Headline News?
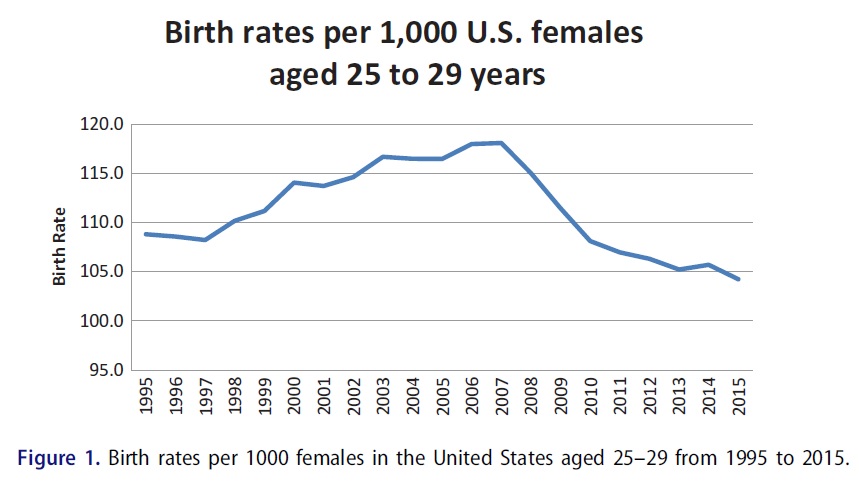
Figure 1 from the study showing increasing birth rates until 2007, and then declining birth rates from the time of the introduction of the Gardasil vaccine to the public.
At the time of the publication of this article, I have not found one single corporate-sponsored “mainstream” news source covering this study.
The fact that fertility rates are decreasing in the U.S. is not a fact that is in dispute. Dr. DeLong begins the article by stating:
The birth rates in the United States for women under the age of 30 are at record lows (Martin, Hamilton, and Osterman 2017). Birth rates per 1,000 females aged 25–29 fell 11.5% from 118.1 in 2007 to 104.5 in 2015. The recent decline follows a steady increase of 8.5% between 1995 and 2006 (from 108.8 to 118).
This decline in birth rates corresponds to the introduction of the HPV vaccine in the U.S.
In 2006, the U.S. Food and Drug Administration (2006) licensed the first of two vaccines to protect women against the human papillomavirus (HPV). Both HPV vaccines (Gardasil and Cevarix) address HPV 16 and 18, two strains of HPV that produce approximately 70% of cervical cancer cases.
The vaccine is recommended for females (and since 2011 for males) aged 11–26.
Dr. DeLong then references studies and cases where premature ovarian failure (POF) was reported after administering the Gardasil vaccine, as well as other symptoms related to infertility.
Reports of young women experiencing primary or premature ovarian failure (POF) after receiving the vaccine were noted (Colafrancesco et al. 2013;Little and Ward 2012, 2014).
Geier and Geier (2017) examined the Vaccine Adverse Events Reporting System (VAERS) database to determine whether uptake of the HPV vaccine affected the number of reports of autoimmune reactions.
VAERS is a passive system where vaccine administrators or recipients report adverse effects after receiving a vaccine.
Between 2006 and 2014, HPV vaccine recipients or their health care providers noted 48 cases of ovarian damage associated with autoimmune reactions.
In addition to the Geier and Geier findings, the VAERS database between 2006 and 2017 indicated other symptoms that affect the ability to bear children: spontaneous abortion (214 cases), amenorrhea (130 cases), and irregular menstruation (123 cases).
Government’s Own Statistics Used to Study 8 Million Women Over 7-Year Period
One of the most compelling aspects of this study is that the researchers used statistics provided by the U.S. government to look at infertility rates.
Data on live births per 1,000 females aged 25–29 originated from the Centers for Disease Control and Prevention (CDC) WONDER database “Births” section: https://wonder.cdc.gov/natality.html. The database reports the numbers starting in 1995.
The number of births is divided by the number of females in the age group using data from WONDER database “Population” section: https://wonder.cdc.gov/bridged-race-population.html. Figure 1 (above) illustrates national numbers from 1995 to 2015.
The chart reveals the steady increase in birth rates through the mid-2000s, followed by a recent sharp decline that is the subject of this analysis.
To analyze possible influences associated with these changes in birth rates, this study examined responses to the National Health and Nutrition Examination Survey (NHANES). The survey collects data on health status of individuals in the United States along with demographic and socioeconomic information.
The National Center for Health Statistic (NCHS) at the CDC administered the survey and selected a representative sample of the US population based upon complex sampling procedure (for details, see https://www.cdc.gov/nchs/nhanes/participant.htm). Data are provided in 2-year cycles.
So the very government agencies responsible for approving the Gardail HPV vaccine, and allowing it to continue to be marketed, namely the CDC and the FDA, provided the data for this study.
Interestingly, and without commentary by the study author, but perhaps well worth noting, the survey questions asked of women changed after the inception of the study in 1995, in 2007, when an additional question was included in the survey:
Starting in 1999, the NHANES asked females aged 12 and up “RHQ131: Has the survey participant ever been pregnant? Please include (current pregnancy,) live births, miscarriages, stillbirths, tubal pregnancies and abortions.”
Responses could be (1) yes, (2) no, (7) refused, (9) don’t know, or (.) missing.
Starting in 2007, the NHANES asked the question to females aged 9 and above, “IMQ040: Has the survey participant ever received one or more doses of the HPV vaccine?”
Response choices were the same as for the pregnancy question.
This begs the question: why did the CDC add the question about HPV vaccination status in 2007 on a pregnancy questionnaire?
Gardasil Vaccine Only Variable that Potentially Explains Decline in Birth Rates
The study author was very careful in her conclusion to state that this study does not prove that the Gardasil HPV vaccine causes women to become infertile. As any scientist knows, correlation does not equal causation.
One common misperception regarding regression analysis is that it may be used to determine causality. Regressions demonstrate associations, not causations.
Although the analysis presented here shows a relationship between vaccine injection and lowered probability of ever being pregnant for females aged 25–29, the conclusion that vaccines were the basis for reduced probability cannot be made.
A second limitation of this analysis is that general probabilities do not imply individual results. That is, even if the probability of becoming pregnant decreased for the group of females who received the HPV vaccine relative to those who did not receive the shot, the findings do not imply that any given female who receives the shot might encounter difficulty conceiving a child.
However, this investigation indicates that more analysis into the HPV shot and fertility is warranted.
Dr. DeLong does, however, look at other factors that could cause infertility in this large study group of over 8 million women, and it is obvious that from the potential causes of infertility, the evidence clearly points to the HPV Gardasil vaccine as the only factor that changed in the study population from 2007 onwards.
Perhaps aggregate birth rates are down due to increased rates of abortion. However, Jatlaoui et al. (2017) reported that for females aged 15–44, the absolute number of abortions, number of abortions per 1,000, and number of abortions per 1,000 live births all steadily declined between 2006 and 2014.
Perhaps enhanced use of contraception contributed to the falling US birth rates. However, Kavanaugh and Jerman (2018) found that the overall utilization of contraception by females aged 15–44 remained at approximately 60% between 2008 and 2014.
Although contraception rates have remained constant, perhaps birth rates were decreased, because birth control improved. Sundaram et al. (2017) confirm that overall contraceptive failure rates (CFR) declined between surveys taken in 2002 and 2006–2010 from 12% to 10%. This decline is particularly interesting, because CFR of most birth control methods were essentially unchanged between 1995 and 2002.
Although overall failure rates fell from 14.9% in 1995 to 12.4% in 2002, that reduction was solely the result of the decline in failure rate of one birth control method, namely withdrawal, from 28% to 18%. The failure rates of all other methods remained
steady during that time period.Perhaps the recession that began in 2008 affected fertility negatively. Using data through 2012, Schneider (2015) noted that fertility fell during the Great Recession that (according to the National Bureau of Economic Research) lasted from 2008 to 2010.
Schneider (2015) demonstrated the effect to be least among older women (aged 35–44) and concluded that the influence of recession on fertility was temporary. If the effect was temporary, the birth rate should climb substantially after the recession as the couples who postponed having children joined the younger couples who wanted to start families.
Figure 2 illustrates that the US employment rates and birth rates tended to move together from 1995 to 2009. However, as employment rates recovered starting in 2010, birth rates continued a slow decline. The Pearson statistic, which measures correlation, was not significant from 1995 to 2015, indicating a lack of relationship between employment and birth rates.
Data suggest that at least part of the reason for the recent decline in US birth rates amongst females aged 25–29 may be associated with increasing injection of the HPV vaccine. (Emphasis added.)
Another alarming statistic Dr. DeLong highlights from the government data is that Gardasil, which was administered in 3 doses during the study period, had a negative correlation on ability to conceive directly related to how many of the 3 doses were injected:
To test whether these results were related to the number of HPV vaccine doses a woman received, the variable that indicated whether a woman received at least one shot was replaced with three variables to indicate the number of shots she received.
If the participant received the HPV vaccine, NHANES included a follow-up question: “IMQ045: How many doses has the survey participant received?”
Table 5 notes that the likelihood of pregnancy diminishes as the number of shots a woman receives increases.
Why Was this Vaccine Ever Approved?
Dr. DeLong addresses the concern about why the dangers of this vaccine were not discovered prior to licensing it:
Questions then arise regarding why the possible link was not found during the safety studies prior to licensing of the vaccine.
We have covered many of these issues in previous articles about Gardasil, but they bear repeating here in the context of this current study.
Flaws in the pre-licensing investigations may have contributed to the lack of findings regarding any effect of the vaccine on reproductive ability of the recipients.
Little and Ward (2014) analyzed the safety studies of the HPV vaccine.
In one safety study, over 50% of the girls enrolled were aged 9–12 years, too young to make observations of changes in menses.
In another study, older girls were required to use contraception, again making effects of the vaccine on fertility difficult to gauge. Follow-up investigations tended to include only adverse events that occurred within 2 weeks of the administration of the vaccine. Although serious adverse events (SAE) were followed for up to 3 years after the vaccine, SAE did not include menstrual abnormalities.
Little and Ward (2014) concluded that safety studies of HPV vaccine did not adequately address the question of ovarian health.
A further possible flaw in the safety investigations involves the placebo. The control groups in some of the clinical trials for HPV vaccines received solutions containing Al (Tomljenovic and Shaw 2013; Tomljenovic, Spinosa, and Shaw 2013) instead of the standard saline solution. The Al itself may produce side effects (Exley 2011) including damage to ovaries (Colafrancesco et al. 2013; Fu et al. 2014).
Finding no marked differences in ovarian function between subjects who received the vaccine and those who received the Al-containing placebo might fail to determine adverse events attributed to Al. The vaccine may negatively affect ovarian function, perhaps through Al in the vaccine (Colafrancesco et al. 2013).
Conclusion: We Have a Public Health Crisis in the U.S. Related to Fertility Rates Among Young Women
Dr. DeLong wants more studies done on the HPV vaccine:
Long-term studies of girls and women who receive the HPV vaccine are warranted. Specifically, investigations need to be undertaken into whether vaccine recipients experience any changes in their menses and ability to conceive. Care needs to be taken so that females taking the birth control pill (or any other intervention that interferes with menstrual cycles) are not included or at least examined separately. Such interventions mask the existence of POF.
Her conclusion that if all the women in the study had received the Gardasil vaccine it would have potentially resulted in 2 million more women unable to conceive children is quite chilling.
This study analyzed survey data that represented nearly 8 million women aged 25–29 living in the United States between 2007 and 2014.
Approximately 60% of women who did not receive the HPV vaccine had been pregnant at least once, whereas only 35% of women who were exposed to the vaccine had ever conceived.
For married women, 75% of the group not exposed to the HPV vaccine conceived, while only 50% of the exposed group had been pregnant at least once.
Results suggest if 100% of the females in this study had received the HPV shot, the number of women who had ever been pregnant would have fallen by 2 million.
Logistic regression analysis revealed that females who received at least one HPV shot were less likely to have ever been pregnant than females who received no shots.
The model controlled for age, relative wealth, college education, ethnicity, and race of the participant. Although safety studies of the HPV vaccine found no significant link to lowered fertility, the design of the investigations may have missed side effects.

Young women whose lives were destroyed by the HPV vaccine.
California Nurse Gives Gardasil Vaccine to Own Daughter who Develops Leukemia and Dies
Infant Accidentally Vaccinated with Gardasil – Mother Blamed for Vaccine Injuries and Baby Medically Kidnapped
Iowa Girl Faces Death: Life Destroyed by Gardasil Vaccine
Gardasil Vaccine Given without Consent and Ruins Life of 14 Year Old Girl
After 3 Years of Suffering 19 Year Old Girl Dies from Gardasil Vaccine Injuries
Gardasil: The Decision We Will Always Regret
The Gardasil Vaccine After-Life: My Daughter is a Shadow of Her Former Self
Gardasil: An Experience no Child Should Have to Go Through
I Want my Daughter’s Life Back the Way it was Before Gardasil
Gardasil Vaccine: Destroyed and Abandoned
15-Year-Old Vaccinated by Force with Gardasil now Suffers from Paralysis and Pain
Recovering from my Gardasil Vaccine Nightmare
Gardasil: We Thought It Was The Right Choice
“HPV Vaccine Has Done This to My Child”
13 Year Old World Championship Karate Student Forced to Quit After Gardasil Vaccine
If I Could Turn Back Time, Korey Would not Have Received any Gardasil Shots
What Doctors Don’t Tell You: Our Gardasil Horror Story
Family Fights U.S. Government over Compensation for Gardasil Vaccine Injuries
Gardasil: When Will our Nightmare End?
HPV Vaccine Injuries: “I Cannot Begin to Describe What it is Like to Watch your Daughter Live in Such Agony”
Gardasil: Don’t Let Your Child Become “One Less”
The Gardasil Vaccine Changed Our Definition of “Normal”
Gardasil: I Should Have Researched First
“They’ve Been Robbed of Their Womanhood” – Local Milwaukee Media Covers Gardasil Vaccine Injuries
Gardasil: The Day Our Daughter’s Life Changed
Gardasil: The Decision I will Always Regret
Gardasil Vaccine: One More Girl Dead
Gardasil: A Parent’s Worst Nightmare
After Gardasil: I Simply Want my Healthy Daughter Back
Gardasil: My Family Suffers with Me
Gardasil Changed my Health, my Life, and Family’s Lives Forever
Gardasil: Ashlie’s Near-Death Experience
Gardasil: My Daughter’s Worst Nightmare
My Personal Battle After the Gardasil Vaccine
Gardasil: The Worst Thing That Ever Happened to Me
A Ruined Life from Gardasil
HPV Vaccines: My Journey Through Gardasil Injuries
The Dark Side of Gardasil – A Nightmare that Became Real
Toddler Wrongly Injected with Gardasil Vaccine Develops Rare Form of Leukaemia
More information about Gardasil

Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
Medical Doctors Opposed to Forced Vaccinations – Should Their Views be Silenced?

One of the biggest myths being propagated in the compliant mainstream media today is that doctors are either pro-vaccine or anti-vaccine, and that the anti-vaccine doctors are all “quacks.”
However, nothing could be further from the truth in the vaccine debate. Doctors are not unified at all on their positions regarding “the science” of vaccines, nor are they unified in the position of removing informed consent to a medical procedure like vaccines.
The two most extreme positions are those doctors who are 100% against vaccines and do not administer them at all, and those doctors that believe that ALL vaccines are safe and effective for ALL people, ALL the time, by force if necessary.
Very few doctors fall into either of these two extremist positions, and yet it is the extreme pro-vaccine position that is presented by the U.S. Government and mainstream media as being the dominant position of the medical field.
In between these two extreme views, however, is where the vast majority of doctors practicing today would probably categorize their position. Many doctors who consider themselves “pro-vaccine,” for example, do not believe that every single vaccine is appropriate for every single individual.
Many doctors recommend a “delayed” vaccine schedule for some patients, and not always the recommended one-size-fits-all CDC childhood schedule. Other doctors choose to recommend vaccines based on the actual science and merit of each vaccine, recommending some, while determining that others are not worth the risk for children, such as the suspect seasonal flu shot.
These doctors who do not hold extreme positions would be opposed to government-mandated vaccinations and the removal of all parental exemptions.
In this article, I am going to summarize the many doctors today who do not take the most extremist pro-vaccine position, which is probably not held by very many doctors at all, in spite of what the pharmaceutical industry, the federal government, and the mainstream media would like the public to believe.

2 Comments